Recurred Macrodystrophia Lipomatosa of the Foot: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Dong-A University Hospital, Busan, Korea. crush06@naver.com
- KMID: 2158426
- DOI: http://doi.org/10.14193/jkfas.2016.20.1.32
Abstract
- We reported on a rare case of recurred macrodystrophia lipomatosa of the foot, and reviewed the literature. A 62-year-old male patient presented with right foot second toe pain; preoperative magnetic resonance imaging and radiograph examination was performed. After surgery the biopsy confirmed the diagnosis. American Orthopaedic Foot and Ankle Society score was checked before and after surgery. Wide excision of the affected area including ray amputation is an effective way to prevent recurrence and relieve the pain after surgery. The 2nd toe ray amputation was performed in the treatment of recurred macrodystrophia lipomatosa of the foot, and is thought to be an effective way to relieve pain and prevent recurrence. After minimally invasive surgery with complete excision surgery, additional data on recurrence and pain relief rate are needed.
Keyword
MeSH Terms
Figure
-

Figure 1. Photograph shows 8×5 cm sized mass on amputated 2nd toe.

Figure 2. Weight-bearing anteroposterior radiograph shows enlarged mass around the right 2nd matatarsophalangeal joint.
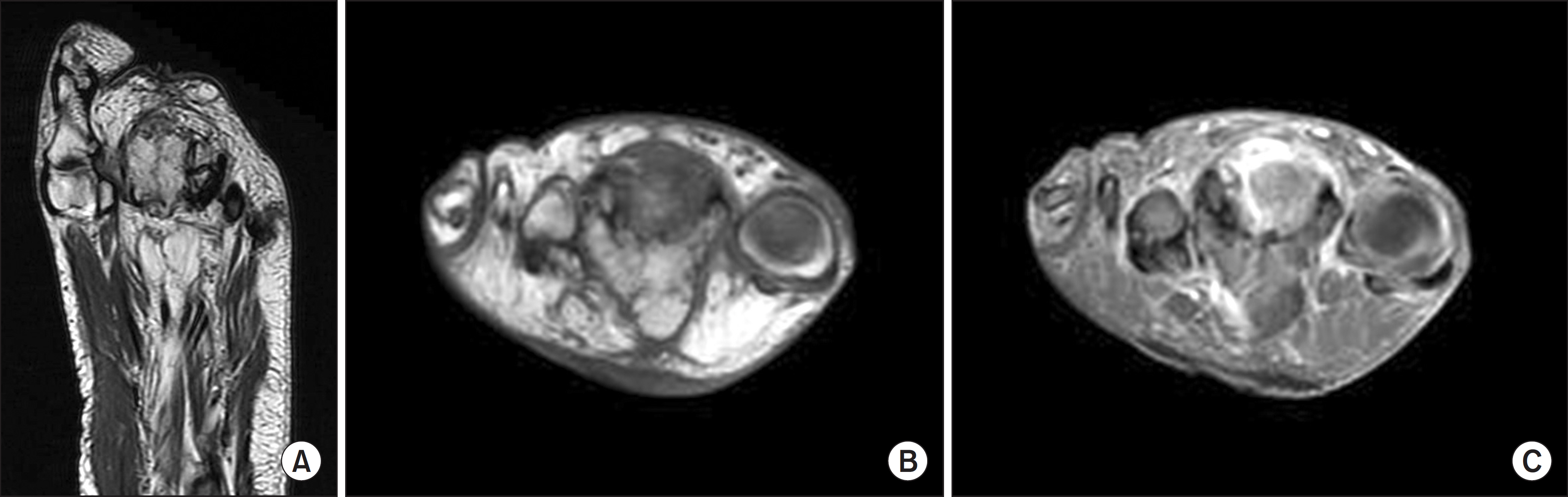
Figure 3. (A) T1-weighted axial magnetic resonance imaging shows enlarged soft tissue around proximal phalanx. (B) The enlarge soft tissue mass has similar signal intensity with around normal fatty tissue in T1-weighted coronal image. (C) T2-weighted coronal image shows slightly high signal intensity around 2nd phalanx and soft tissue mass.
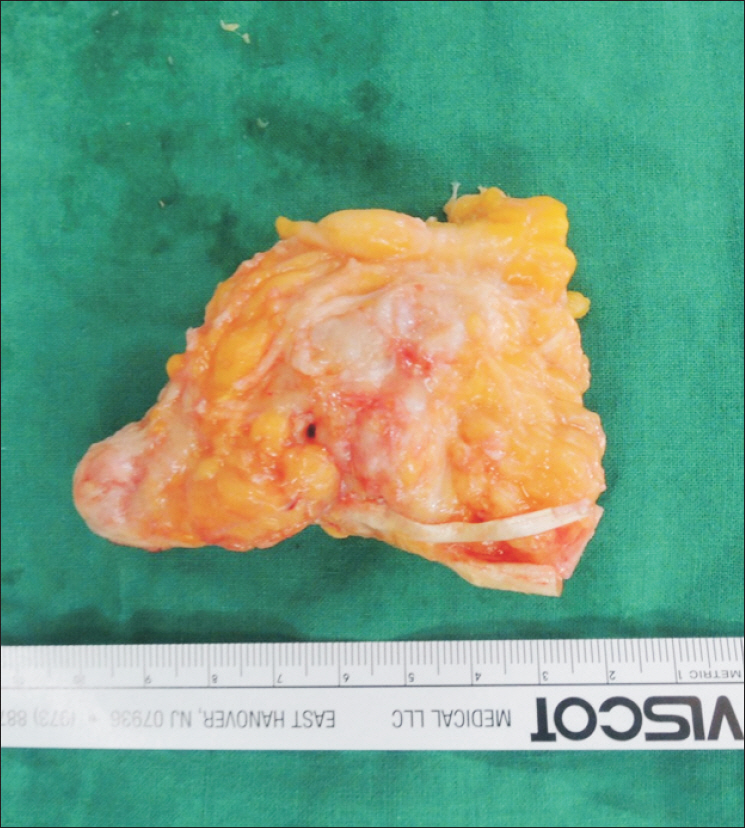
Figure 4. Intraoperative finding shows fibrofatty tissue. The histologic examination of the removed tissue shows 8×5 cm in dimension.
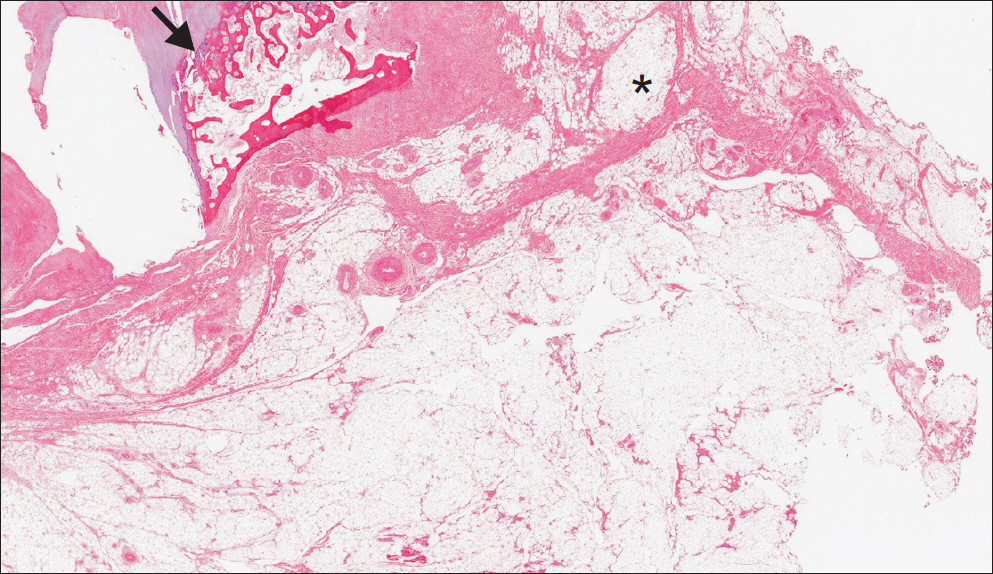
Figure 5. Histological finding (H&E stain, ×10). The outer surface attached with fibroadipose tissue and some nerve bundles was seen (asterisk). Focal necrosis with woven bone formation in medulla and fibroadipose tissue overgrowth around the bone was seen (arrow).

Figure 6. Postoperative 1 year, anteroposterior radiograph shows ray amputated 2nd toe.
Reference
-
References
1. Barsky AJ. Macrodactyly. J Bone Joint Surg Am. 1967; 49:1255–66.
Article2. Denaro V, Papapietro N, Gulino G. Macrodystrophia lipomatosa of the foot: case report and surgical treatment. Eur J Orthop Surg Traumatol. 1999; 9:61–4.3. D'Costa H, Hunter JD, O'Sullivan G, O'Keefe D, Jenkins JP, Hughes PM. Magnetic resonance imaging in macromelia and macrodactyly. Br J Radiol. 1996; 69:502–7.4. Moran V, Butler F, Colville J. X-ray diagnosis of macrodystrophia lipomatosa. Br J Radiol. 1984; 57:523–5.
Article5. Baruchin AM, Herold ZH, Shmueli G, Lupo L. Macrodystrophia lipomatosa of the foot. J Pediatr Surg. 1988; 23:192–4.
Article6. Blacksin M, Barnes FJ, Lyons MM. MR diagnosis of macrodystrophia lipomatosa. AJR Am J Roentgenol. 1992; 158:1295–7.
Article7. Brodwater BK, Major NM, Goldner RD, Layfield LJ. Macrodystrophia lipomatosa with associated fibrolipomatous hamartoma of the median nerve. Pediatr Surg Int. 2000; 16:216–8.
Article8. Prasetyono TO, Hanafi E, Astriana W. A review of macrodystrophia lipomatosa: revisitation. Arch Plast Surg. 2015; 42:391–406.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Macrodystrophia Lipomatosa of the Foot (A Case Report)
- Surgical Treatment of Macrodystrophia Lipomatosa Involving Superficial Peroneal Nerve in the Foot and Ankle
- Macrodystrophia Lipomatosa: One Case Report
- Macrodystrophia lipomatosa
- Macrodystrophia lipomatosa of bilateral hands and the left upper limb with syndactyly
