J Korean Med Sci.
2011 Mar;26(3):386-391. 10.3346/jkms.2011.26.3.386.
The Relationship between Normal Serum Uric Acid and Nonalcoholic Fatty Liver Disease
- Affiliations
-
- 1Department of Family Medicine, Gachon University Gil Medical Center, Incheon, Korea.
- 2Department of Medicine, Dongguk University, Seoul, Korea. fmmodel@gmail.com
- 3Department of Statistics, Dongguk University, Seoul, Korea.
- KMID: 2157876
- DOI: http://doi.org/10.3346/jkms.2011.26.3.386
Abstract
- The objective of the present study was to determine the relationship between serum uric acid (SUA) level and the presence of nonalcoholic fatty liver disease (NAFLD). We analyzed data of 9,019 Koreans who visited a health check up center. The SUA levels of all of these subjects were within the normal range. The participants were divided into 4 groups according to the quartiles of the SUA levels for both sexes. Hepatic steatosis was diagnosed on the basis of ultrasonographic findings. Multivariate logistic regression modeling was performed across the SUA quartiles. The presence of NAFLD and metabolic abnormalities were found significantly in subjects with high-normal SUA levels. After adjustment for age, metabolic components, and the liver-function test, the adjusted odds ratio (OR, 95% CIs) for the presence of NAFLD in the subjects with the highest SUA level was 1.46 (1.17-1.82) for men and 2.13 (1.42-3.18) for women, as compared to the subjects with the lowest SUA level. Our results suggest that increased SUA concentrations, even within the normal range, are independently associated with the presence of NAFLD.
MeSH Terms
Figure
-
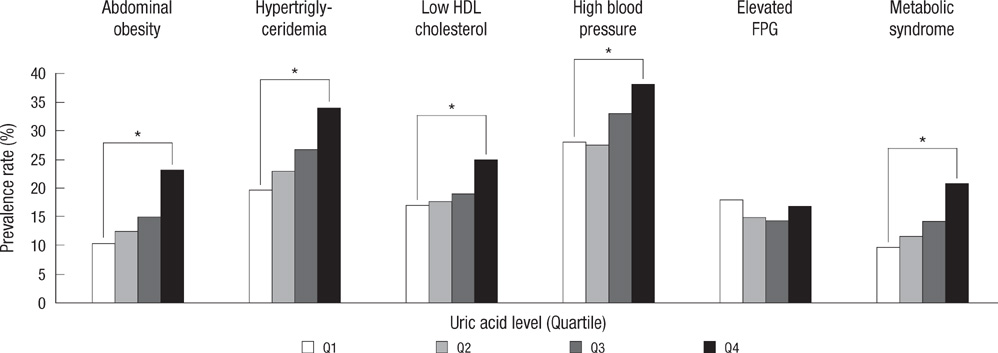
Fig. 1 Prevalences of metabolic syndrome (MS) and each component of MS according to the serum uric acid (SUA) quartiles. Metabolic syndrome was defined as having 3 or more of the following criteria: an waist circumference of ≥ 90 cm for men and ≥ 85 cm for women; a triglyceride level of ≥ 150 mg/dL; HDL cholesterol < 40 mg/dL for men and < 50 mg/dL for women; blood pressure ≥ 130/85 mmHg or receiving antihypertensive drugs; fasting plasma glucose (FPG) ≥ 100 mg/dL or receiving antidiabetic medication. *P for trend < 0.05.
Reference
-
1. Caballería L, Auladell MA, Torán P, Miranda D, Aznar J, Pera G, Gil D, Muñoz L, Planas J, Canut S, Bernad J, Aubà J, Pizarro G, Aizpurua MM, Altaba A, Tibau A. Prevalence and factors associated with the presence of non alcoholic fatty liver disease in an apparently healthy adult population in primary care units. BMC Gastroenterol. 2007. 7:41–46.2. Angulo P. Nonalcoholic fatty liver disease. N Engl J Med. 2002. 346:1221–1231.3. Assy N, Kaita K, Mymin D, Levy C, Rosser B, Minuk G. Fatty infiltration of liver in hyperlipidemic patients. Dig Dis Sci. 2000. 45:1929–1934.4. Gupte P, Amarapurkar D, Agal S, Baijal R, Kulshrestha P, Pramanik S, Patel N, Madan A, Amarapurkar A, Hafeezunnisa . Non-alcoholic steatohepatitis in type 2 diabetes mellitus. J Gastroenterol Hepatol. 2004. 19:854–858.5. Marchesini G, Brizi M, Bianchi G, Tomassetti S, Bugianesi E, Lenzi M, McCullough AJ, Natale S, Forlani G, Melchionda N. Nonalcoholic fatty liver disease: a feature of the metabolic syndrome. Diabetes. 2001. 50:1844–1850.6. Fauci AS, Harrison TR. Harrison's principles of internal medicine. 2008. 17th ed. New York; London: McGraw-Hill Medical;2444.7. Feig DI, Kang DH, Johnson RJ. Uric acid and cardiovascular risk. N Engl J Med. 2008. 359:1811–1821.8. Lee K. Relationship between uric acid and hepatic steatosis among Koreans. Diabetes Metab. 2009. 35:447–451.9. Lee YJ, Lee HR, Lee JH, Shin YH, Shim JY. Association between serum uric acid and non-alcoholic fatty liver disease in Korean adults. Clin Chem Lab Med. 2010. 48:175–180.10. Li Y, Xu C, Yu C, Xu L, Miao M. Association of serum uric acid level with non-alcoholic fatty liver disease: a cross-sectional study. J Hepatol. 2009. 50:1029–1034.11. World Health Organization. Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1995. 854:1–452.12. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, Smith SC Jr, Spertus JA, Costa F. American Heart Association. National Heart, Lung, and Blood Institute. Diagnosis and management of the metabolic syndrome: an Ameri can Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005. 112:2735–2752.13. Lee SY, Park HS, Kim DJ, Han JH, Kim SM, Cho GJ, Kim DY, Kwon HS, Kim SR, Lee CB, Oh SJ, Park CY, Yoo HJ. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res Clin Pract. 2007. 75:72–80.14. Browning JD, Szczepaniak LS, Dobbins R, Nuremberg P, Horton JD, Cohen JC, Grundy SM, Hobbs HH. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology. 2004. 40:1387–1395.15. Sonsuz A, Basaranoglu M, Ozbay G. Relationship between aminotransferase levels and histopathological findings in patients with nonalcoholic steatohepatitis. Am J Gastroenterol. 2000. 95:1370–1371.16. Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. N Engl J Med. 2000. 342:1266–1271.17. Niskanen LK, Laaksonen DE, Nyyssönen K, Alfthan G, Lakka HM, Lakka TA, Salonen JT. Uric acid level as a risk factor for cardiovascular and all-cause mortality in middle-aged men: a prospective cohort study. Arch Intern Med. 2004. 164:1546–1551.18. Lehto S, Niskanen L, Rönnemaa T, Laakso M. Serum uric acid is a strong predictor of stroke in patients with non-insulin-dependent diabetes mellitus. Stroke. 1998. 29:635–639.19. Jung DH, Lee YJ, Lee HR, Lee JH, Shim JY. Association of renal manifestations with serum uric acid in Korean adults with normal uric acid levels. J Korean Med Sci. 2010. 25:1766–1770.20. Day CP, James OF. Steatohepatitis: a tale of two "hits"? Gastroenterology. 1998. 114:842–845.21. Quiñones Galvan A, Natali A, Baldi S, Frascerra S, Sanna G, Ciociaro D, Ferrannini E. Effect of insulin on uric acid excretion in humans. Am J Physiol. 1995. 268:E1–E5.22. Modan M, Halkin H, Karasik A, Lusky A. Elevated serum uric acid--a facet of hyperinsulinaemia. Diabetologia. 1987. 30:713–718.23. Nakagawa T, Tuttle KR, Short RA, Johnson RJ. Hypothesis: fructose-induced hyperuricemia as a causal mechanism for the epidemic of the metabolic syndrome. Nat Clin Pract Nephrol. 2005. 1:80–86.24. Dawson J, Walters M. Uric acid and xanthine oxidase: future therapeutic targets in the prevention of cardiovascular disease? Br J Clin Pharmacol. 2006. 62:633–644.25. Johnson RJ, Kang DH, Feig D, Kivlighn S, Kanellis J, Watanabe S, Tuttle KR, Rodriguez-Iturbe B, Herrera-Acosta J, Mazzali M. Is there a pathogenetic role for uric acid in hypertension and cardiovascular and renal disease? Hypertension. 2003. 41:1183–1190.26. Ruggiero C, Cherubini A, Ble A, Bos AJ, Maggio M, Dixit VD, Lauretani F, Bandinelli S, Senin U, Ferrucci L. Uric acid and inflammatory markers. Eur Heart J. 2006. 27:1174–1181.27. Saverymuttu SH, Joseph AE, Maxwell JD. Ultrasound scanning in the detection of hepatic fibrosis and steatosis. Br Med J (Clin Res Ed). 1986. 292:13–15.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Noninvasive serum biomarkers for liver steatosis in nonalcoholic fatty liver disease: Current and future developments
- The Clinical Significance of Hypouricemia in Patients with Liver Cirrhosis
- Predictors Related to the Non-alcoholic Fatty Liver Disease
- Elevated serum bilirubin levels are inversely associated with nonalcoholic fatty liver disease
- Serum Uric Acid as a Predictor for the Development of Nonalcoholic Fatty Liver Disease in Apparently Healthy Subjects: A 5-Year Retrospective Cohort Study
