ST-Segment Elevation Myocardial Infarction as a Result of Coronary Artery Ectasia-Related Intracoronary Thrombus in a Patient with Liver Cirrhosis
- Affiliations
-
- 1Department of Internal Medicine, Bucheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Bucheon, Korea. sungmin@catholic.ac.kr
- KMID: 2156195
- DOI: http://doi.org/10.4266/kjccm.2015.30.4.358
Abstract
- Coronary artery ectasia (CAE) is a rare condition defined as the dilatation of coronary artery to at least 1.5 times larger than the normal adjacent coronary artery. Clinical manifestations of CAE vary, ranging from asymptomatic to ST-segment elevation myocardial infarction (STEMI). Because of its rarity and clinical diversity, the best treatment strategy and prognosis for CAE remain unclear. We describe a case of STEMI caused by intracoronary thrombus formation within an ectatic area in a patient with liver cirrhosis (LC). The patient was successfully managed by thrombus aspiration only, without balloon angioplasty or stent implantation, and maintained by dual antiplatelet therapy with aspirin and ticagrelor, a potent new P2Y12 inhibitor.
Keyword
MeSH Terms
Figure
-
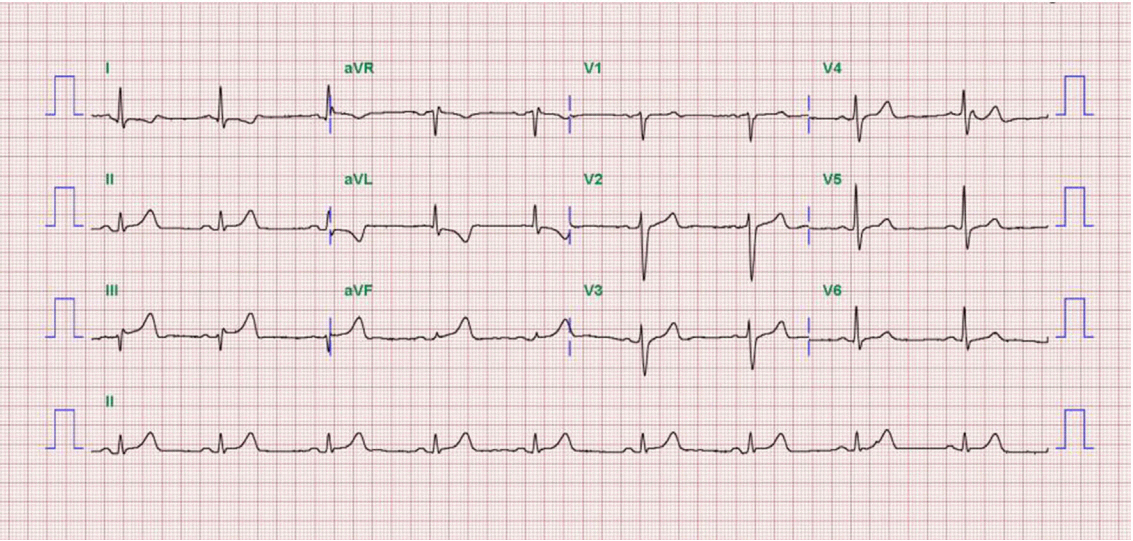
Fig. 1. Electrocardiograms at admission shows ST-segment elevation on the ll, lll, and aVF leads with reciprocal change on the I and aVL leads.
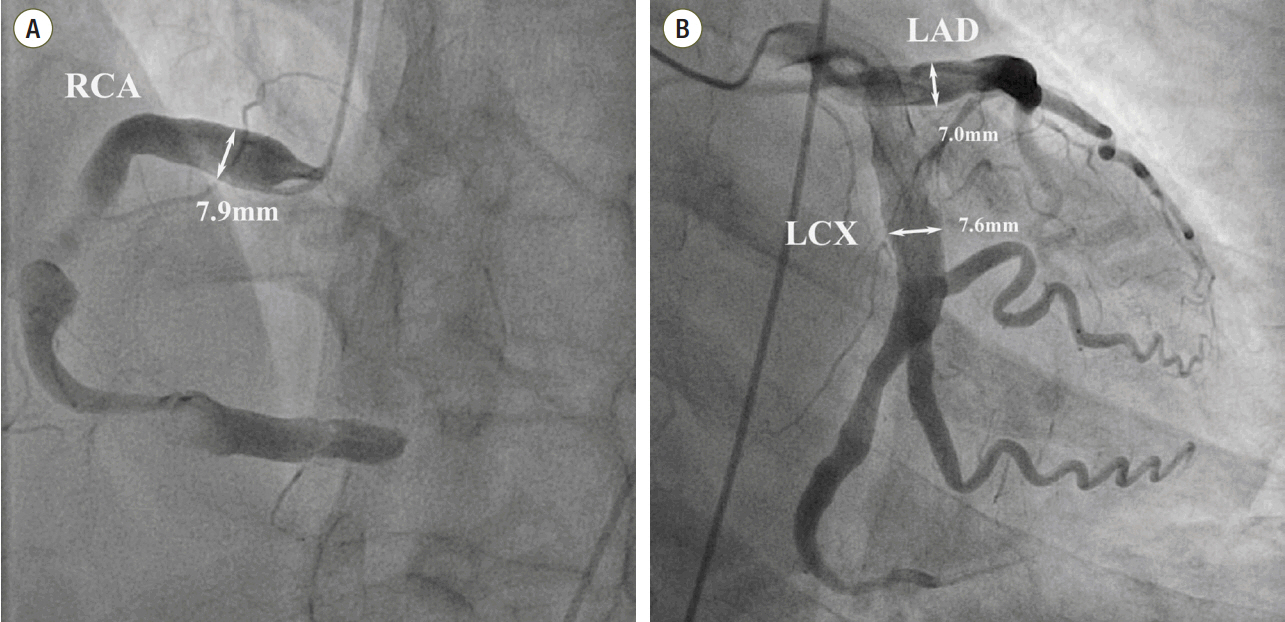
Fig. 2. Coronary angiography shows severe ectatic dilatation in all 3 mojor epicardial coronary arteries. (A) Distal right coronary artery was totally occluded by thrombus. Proximal right coronary artery segment diameter is 7.9 mm, (B) proximal left anterior descending coronary artery segment diameter is 7.0 mm and the proximal left circumflex coronary artery is 7.6 mm. RCA: right coronary artery; LAD: left anterior descending coronary artery; LCX: left circumflex coronary artery.
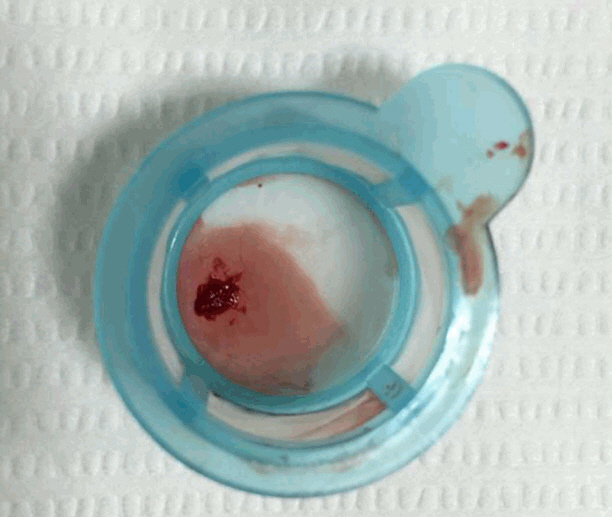
Fig. 3. There are aspirated red thrombi by thrombosuction device.

Fig. 4. After thrombosuction, right coronary artery flow was totally recovered.
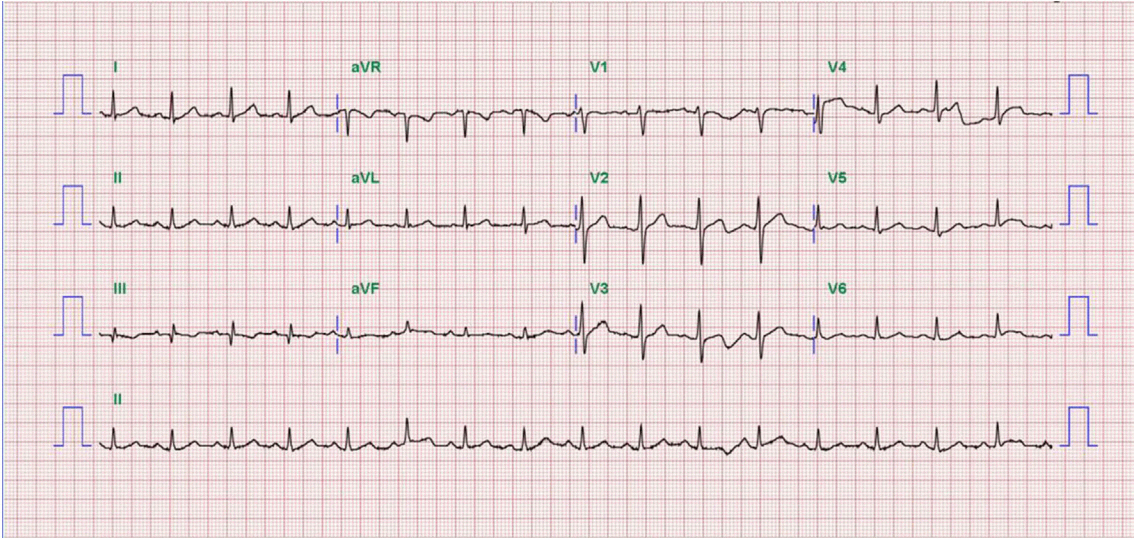
Fig. 5. Electrocardiogram one day after thrombosuction shows ST-segment resolution on II, III, and aVF leads.
Reference
-
References
1. Swaye PS, Fisher LD, Litwin P, Vignola PA, Judkins MP, Kemp HG, et al. Aneurysmal coronary artery disease. Circulation. 1983; 67:134–8.
Article2. Manginas A, Cokkinos DV. Coronary artery ectasias: imaging, functional assessment and clinical implications. Eur Heart J. 2006; 27:1026–31.
Article3. Demopoulos VP, Olympios CD, Fakiolas CN, Pissimissis EG, Economides NM, Adamopoulou E, et al. The natural history of aneurysmal coronary artery disease. Heart. 1997; 78:136–41.
Article4. Yetkin E, Waltenberger J. Novel insights into an old controversy: is coronary artery ectasia a variant of coronary atherosclerosis? Clin Res Cardiol. 2007; 96:331–9.5. Otsubo R, Higuchi Mde L, Gutierrez PS, Benvenuti LA, Massarollo PC, Costa AL, et al. Influence of chronic liver disease on coronary atherosclerosis vulnerability features. Int J Cardiol. 2006; 109:387–91.
Article6. Movahed MR, John J, Hashemzadeh M, Jamal MM, Hashemzadeh M. Trends in the age adjusted mortality from acute ST segment elevation myocardial infarction in the United States (1988-2004) based on race, gender, infarct location and comorbidities. Am J Cardiol. 2009; 104:1030–4.
Article7. al-Harthi SS, Nouh MS, Arafa M, al-Nozha M. Aneurysmal dilatation of the coronary arteries: diagnostic patterns and clinical significance. Int J Cardiol. 1991; 30:191–4.
Article8. Printz BF, Sleeper LA, Newburger JW, Minich LL, Bradley T, Cohen MS, et al. Noncoronary cardiac abnormalities are associated with coronary artery dilation and with laboratory inflammatory markers in acute Kawasaki disease. J Am Coll Cardiol. 2011; 57:86–92.
Article9. Dahhan A. Coronary artery ectasia in atherosclerotic coronary artery disease, inflammatory disorders, and sickle cell disease. Cardiovasc Ther. 2015; 33:79–88.
Article10. Pinar Bermúdez E, López Palop R, Lozano Martínez-Luengas I, Cortés Sánchez R, Carrillo Sáez P, Rodrí-guez Carreras R, et al. Coronary ectasia: prevalence, and clinical and angiographic characteristics. Rev Esp Cardiol. 2003; 56:473–9.11. Mendelsohn ME, Karas RH. The protective effects of estrogen on the cardiovascular system. N Engl J Med. 1999; 340:1801–11.
Article12. Castilla A, Prieto J, Fausto N. Transforming growth factors beta 1 and alpha in chronic liver disease. Effects of interferon alfa therapy. N Engl J Med. 1991; 324:933–40.13. Arjal R, Trotter JF. International normalized ratio of prothrombin time in the model for end-stage liver disease score: an unreliable measure. Clin Liver Dis. 2009; 13:67–71.14. Krüger D, Stierle U, Herrmann G, Simon R, Sheikhzadeh A. Exercise-induced myocardial ischemia in isolated coronary artery ectasias and aneurysms (“dilated coronopathy”). J Am Coll Cardiol. 1999; 34:1461–70.15. Authors/Task Force Members, Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2015; [Epub ahead of print].16. Tsochatzis EA, Bosch J, Burroughs AK. New therapeutic paradigm for patients with cirrhosis. Hepatology. 2012; 56:1983–92.
Article17. Ge PS, Runyon BA. The changing role of beta-blocker therapy in patients with cirrhosis. J Hepatol. 2014; 60:643–53.
Article18. Vijayanagar R, Shafii E, DeSantis M, Waters RS, Desai A. Surgical treatment of coronary aneurysms with and without rupture. J Thorac Cardiovasc Surg. 1994; 107:1532–5.
Article19. Oh SK, Rha SW, Kook H, Kim DH, Ho SY, Kim SH, et al. Two different successful angioplasty methods in patients with stenotic coronary artery ectasia. Chonnam Med J. 2012; 48:185–9.
Article20. Echavarría-Pinto M, Lopes R, Gorgadze T, Gonzalo N, Hernández R, Jiménez-Quevedo P, et al. Safety and efficacy of intense antithrombotic treatment and percutaneous coronary intervention deferral in patients with large intracoronary thrombus. Am J Cardiol. 2013; 111:1745–50.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Simultaneous Total Occlusion of Multiple Distal Coronary Arteries in Acute Myocardial Infarction
- No-Reflow Phoenomenon by Intracoronary Thrombus in Acute Myocardial Infarction
- Acute Myocardial Infarction by Right Coronary Artery Occlusion Presenting as Precordial ST Elevation on Electrocardiography
- A case of acute anterior and lateral myocardial infarction altering with time from a large intracoronary thrombus on left main trunk
- A Case of Gigantic Ectasia of Right Coronary Artery Associated with Acute Myocardial Infarction
