Korean J Neurotrauma.
2013 Oct;9(2):125-130. 10.13004/kjnt.2013.9.2.125.
The Clinical Course of Subdural Hygroma with Head Injury
- Affiliations
-
- 1Department of Neurosurgery, Hallym University College of Medicine, Kangnam Sacred Heart Hospital, Seoul, Korea. nskch@hallym.or.kr
- KMID: 2156113
- DOI: http://doi.org/10.13004/kjnt.2013.9.2.125
Abstract
OBJECTIVE
Traumatic subdural hygroma (T-SDG) has been generally treated using conservative management rather than surgical methods. This study was performed to evaluate the clinical course of T-SDG with radiologic studies.
METHODS
A retrospective study was conducted among patients diagnosed with T-SDG from January 2011 to December 2011. The patients were categorized into two groups. Group A has the widest width of T-SDG below 8 mm, Group B more than 8 mm. Computed tomography (CT) and magnetic resonance imaging (MRI) were carried out in both groups.
RESULTS
Seventy-four patients were confirmed with T-SDG and were grouped as follows: 44 patients in Group A and 30 patients in Group B. There was no significant difference in age and sex ratio between group A and B. It took more time to resolve T-SDG in Group B (95.2+/-86.4 days) than Group A (14.4+/-6.7)(p<0.001). However, no significant difference was observed in the Glasgow Coma Scale (GCS) between the groups. In 10 patients of Group B, T-SDG developed into chronic subdural hematoma and one of these patients underwent surgery.
CONCLUSION
Most T-SDGs were resolved after some period in this study. Surgery does not seem to be necessary in resolving T-SDG.
MeSH Terms
Figure
-
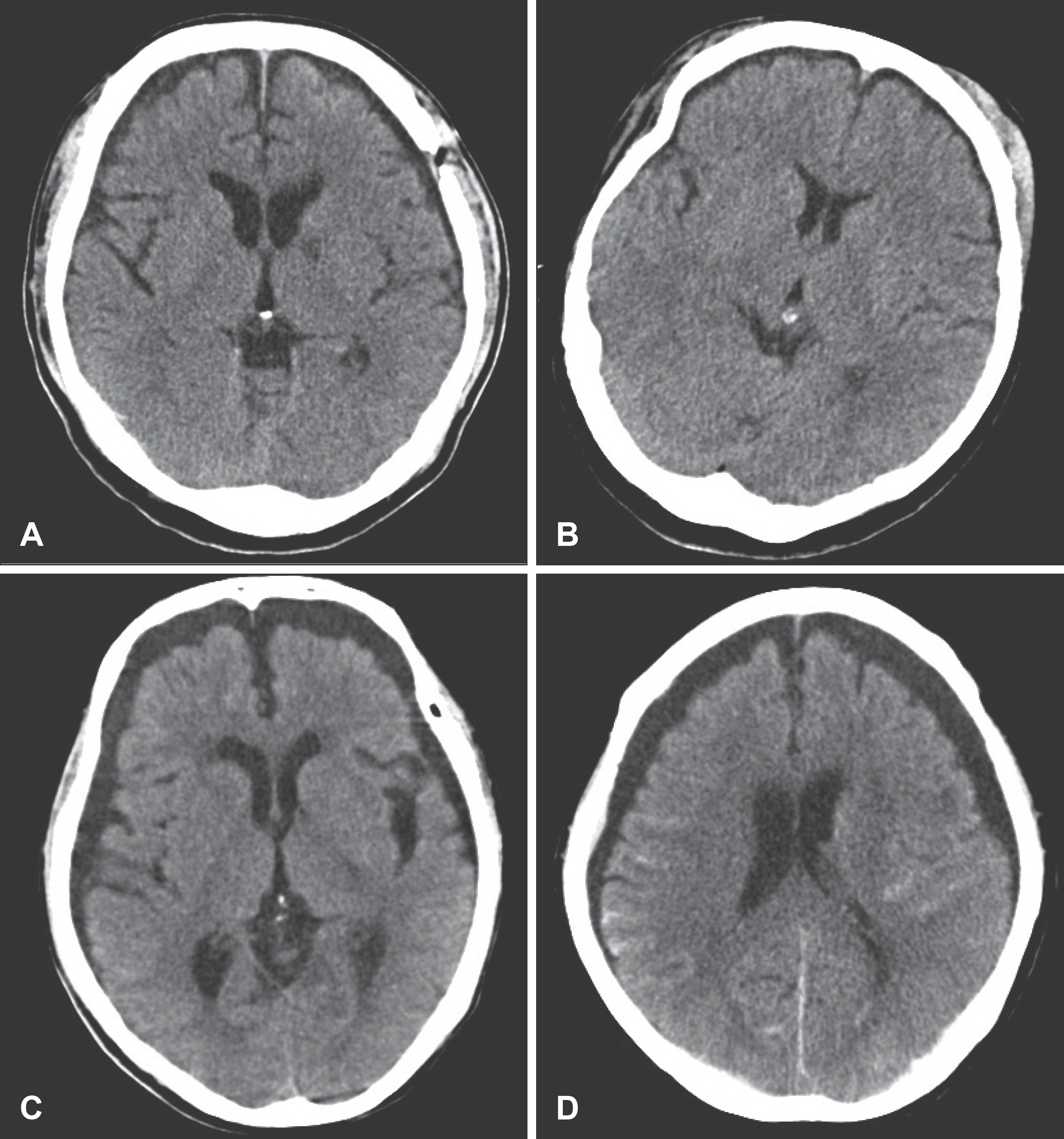
FIGURE 1. CT findings of representative cases. In a group A patient (A and B) the maximum width of T-SDG is below 8 mm whereas it is more than 8 mm in group B (C and D). T-SDG: traumatic subdural hematoma.
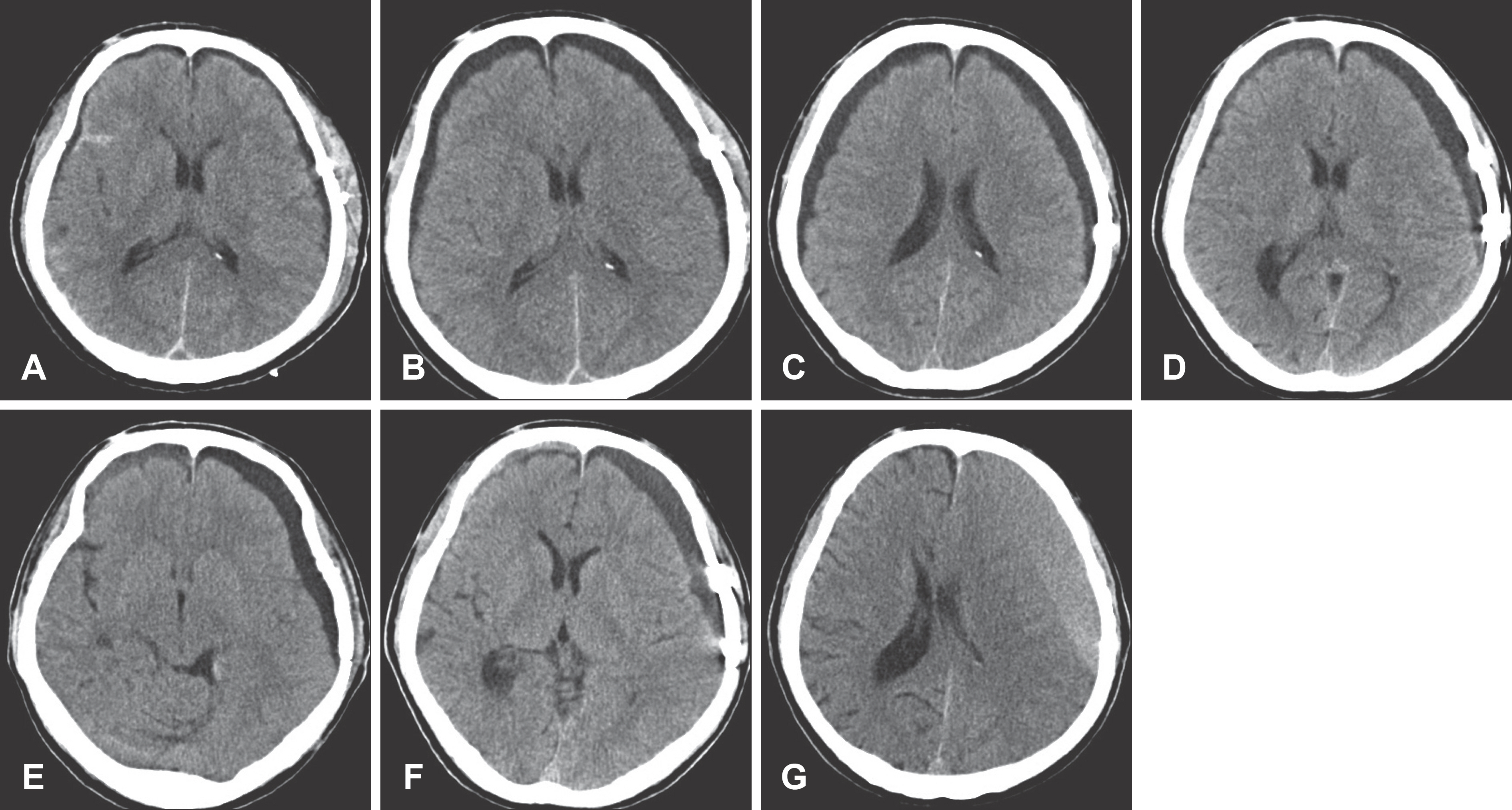
FIGURE 2. The patient of T-SDG who changed to chronic subdural hematoma and was treated by surgical management. He had undergone surgical removal of epidural hematoma (EDH) in second hospital day. A: Post-operative day (POD) 1. B: POD 10. C: POD 27. D: POD 38. E: POD 47. F: POD 90. G: POD 118.
Cited by 1 articles
-
History of Chronic Subdural Hematoma
Kyeong-Seok Lee
Korean J Neurotrauma. 2015;11(2):27-34. doi: 10.13004/kjnt.2015.11.2.27.
Reference
-
References
1. Borzone M, Capuzzo T, Perria C, Rivano C, Tercero E. Traumatic subdural hygromas: a report of 70 surgically treated cases. J Neurosurg Sci. 27:161–165. 1983.2. French BN, Cobb CA 3rd, Corkill G, Youmans JR. Delayed evolution of posttraumatic subdural hygroma. Surg Neurol. 9:145–148. 1978.3. Friede RL, Schachenmayr W. The origin ofsubdural neomembran-es. II. Fine structural of neomembranes. Am J Pathol. 92:69–84. 1978.4. Hasegawa M, Yamashima T, Yamashita J, Suzuki M, Shimada S. Traumatic subdural hygroma: pathology and meningeal enhancement on magnetic resonance imaging. Neurosurgery. 31:580–585. 1992.5. HillL NC, Goldstein NP, McKenzie BF, McGuckin WF, Svien HJ. Cerebrospinal-fluid proteins, glycoproteins, and lipoproteins in obstructive lesions of the central nervous system. Brain. 82:581–593. 1959.
Article6. Hoff J, Bates E, Barnes B, Glickman M, Margolis T. Traumatic subdural hygroma. J Trauma. 13:870–876. 1973.
Article7. Ju CI, Kim SW, Lee SM, Shin H. The surgical results of traumatic subdural hygroma treated with subduroperitoneal shunt. J Korean Neurosurg Soc. 37:436–442. 2005.8. Koizumi H, Fukamachi A, Wakao T, Tasaki T, Nagaseki Y, Yanai Y. [Traumatic subdural hygromas in adults–on the possibility of development of chronic subdural hematoma (author's transl)]. Neurol Med Chir (Tokyo). 21:397–406. 1981.9. Lee KS, Bae WK, Bae HG, Yun IG. The fate of traumatic subdural hygroma in serial computed tomographic scans. J Korean Med Sci. 15:560–568. 2000.
Article10. Lee KS, Bae WK, Park YT, Yun IG. The pathogenesis and fate of traumatic subdural hygroma. Br J Neurosurg. 8:551–558. 1994.
Article11. Lee KS, Doh JW, Bae HG, Yun IG. Relations among traumatic subdural lesions. J Korean Med Sci. 11:55–63. 1996.
Article12. Litofsky NS, Raffel C, McComb JG. Management of symptomat-ic chronic extra-axial fluid collections in pediatric patients. Neurosurgery. 31:445–450. 1992.
Article13. McCluney KW, Yeakley JW, Fenstermacher MJ, Baird SH, Bon-mati CM. Subdural hygroma versus atrophy on MR brain scans: “the cortical vein sign”. AJNR Am J Neuroradiol. 13:1335–1339. 1992.14. McConnell AA. Traumatic subdural effusions. J Neurol Psychiatry. 4:237–256. 1941.
Article15. Naffziger HC. Subdural fluid accumulations following head injury. JAMA. 82:1751–1752. 1924.
Article16. St John JN, Dila C. Traumatic subdural hygroma in adults. Neurosurgery. 9:621–626. 1981.
Article17. Stone JL, Lang RG, Sugar O, Moody RA. Traumatic subdural hygroma. Neurosurgery. 8:542–550. 1981.
Article18. Wetterling T, Demierre B, Rama B, Spoerri O. The clinical course of surgically treated posttraumatic subdural hygromas. Acta Neurochir (Wien). 83:99–104. 1986.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Escherichia Coli Subdural Empyema Following Subdural Hygroma in Elderly Patient
- Chronic Subdural Hematoma Superimposed on Posttraumatic Subdural Hygroma: A Report of Three Cases
- Clinical Analysis of Traumatic Subdural Hygroma
- Clinical Analysis of Subdural Hygroma
- Clinical Evaluation of the Traumatic Subdural Hygroma
