Korean J Urol.
2015 May;56(5):379-385. 10.4111/kju.2015.56.5.379.
The effect of renal cortical thickness on the treatment outcomes of kidney stones treated with shockwave lithotripsy
- Affiliations
-
- 1The S.H. Ho Urology Centre, Department of Surgery, The Chinese University of Hong Kong, Hong Kong, China. ngcf@surgery.cuhk.edu.hk
- 2Department of Imaging and Intervention Radiology, The Chinese University of Hong Kong, Hong Kong, China.
- KMID: 2155318
- DOI: http://doi.org/10.4111/kju.2015.56.5.379
Abstract
- PURPOSE
Because the shock wave passes through various body tissues before reaching the stone, stone composition may affect the treatment efficacy of shock wave lithotripsy (SWL). We investigated the effect of various tissue components along the shock wave path on the success of SWL.
MATERIALS AND METHODS
From October 2008 to August 2010, a total of 206 patients with kidney stones sized 5 to 20 mm were prospectively recruited for a study of the factors that affect the outcome of treatment with a Sonolith Vision lithotripter. Successful SWL was defined as either stone-free status or residual fragments <4 mm at 12 weeks. Logistic regression analysis was performed to assess the factors that predicted treatment outcomes. Potential predictors included the patient's age, shock wave delivery rate, stone volume (SV), mean stone density (MSD), skin-to-stone distance (SSD), and the mean thickness of the three main components along the shock wave path: renal cortical thickness (KT), muscle thickness (MT), and soft-tissue thickness (ST).
RESULTS
The mean age of the patients was 53.8 years (range, 25-82 years). The overall treatment success rate after one session of SWL was 43.2%. The mean KT, MT, and ST were 26.9, 16.6, and 40.8 mm, respectively. The logistic regression results showed that a slower shock wave delivery rate, smaller SV, a lower MSD, and a thicker KT were found to be significant predictors for successful SWL. SSD, MT, and ST were not predictors of successful treatment.
CONCLUSIONS
Among the main tissue components along the shock wave path, a thicker KT was a favorable factor for successful SWL after adjustment for SV, MSD, and the shock wave delivery rate.
Keyword
MeSH Terms
Figure
-
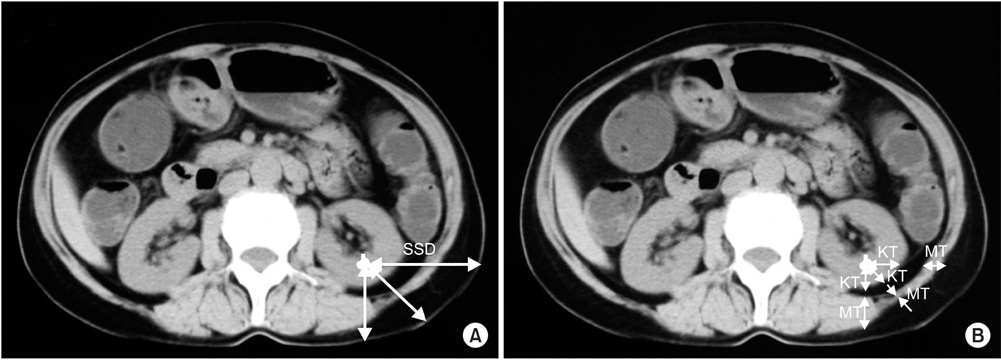
Fig. 1 (A) Measurement of skin-to-stone distance (SSD) at three differently angled paths (0°, 45°, and 90°) from the center of the stone to the skin. (B) Measurement of the renal cortical thickness (KT) and muscle thickness (MT) on the three angled paths.
Reference
-
1. Wiesenthal JD, Ghiculete D, D'A Honey RJ, Pace KT. Evaluating the importance of mean stone density and skin-to-stone distance in predicting successful shock wave lithotripsy of renal and ureteric calculi. Urol Res. 2010; 38:307–313.2. Ng CF, Siu DY, Wong A, Goggins W, Chan ES, Wong KT. Development of a scoring system from noncontrast computerized tomography measurements to improve the selection of upper ureteral stone for extracorporeal shock wave lithotripsy. J Urol. 2009; 181:1151–1157.3. Pareek G, Hedican SP, Lee FT Jr, Nakada SY. Shock wave lithotripsy success determined by skin-to-stone distance on computed tomography. Urology. 2005; 66:941–944.4. El-Nahas AR, El-Assmy AM, Mansour O, Sheir KZ. A prospective multivariate analysis of factors predicting stone disintegration by extracorporeal shock wave lithotripsy: the value of high-resolution noncontrast computed tomography. Eur Urol. 2007; 51:1688–1693.5. Perks AE, Schuler TD, Lee J, Ghiculete D, Chung DG, D'A Honey RJ, et al. Stone attenuation and skin-to-stone distance on computed tomography predicts for stone fragmentation by shock wave lithotripsy. Urology. 2008; 72:765–769.6. Kacker R, Zhao L, Macejko A, Thaxton CS, Stern J, Liu JJ, et al. Radiographic parameters on noncontrast computerized tomography predictive of shock wave lithotripsy success. J Urol. 2008; 179:1866–1871.7. Jacobs BL, Smaldone MC, Smaldone AM, Ricchiuti DJ, Averch TD. Effect of skin-to-stone distance on shockwave lithotripsy success. J Endourol. 2008; 22:1623–1627.8. Patel T, Kozakowski K, Hruby G, Gupta M. Skin to stone distance is an independent predictor of stone-free status following shockwave lithotripsy. J Endourol. 2009; 23:1383–1385.9. Park YI, Yu JH, Sung LH, Noh CH, Chung JY. Evaluation of possible predictive variables for the outcome of shock wave lithotripsy of renal stones. Korean J Urol. 2010; 51:713–718.10. Juan HC, Lin HY, Chou YH, Yang YH, Shih PM, Chuang SM, et al. Abdominal fat distribution on computed tomography predicts ureteric calculus fragmentation by shock wave lithotripsy. Eur Radiol. 2012; 22:1624–1630.11. Park BH, Choi H, Kim JB, Chang YS. Analyzing the effect of distance from skin to stone by computed tomography scan on the extracorporeal shock wave lithotripsy stone-free rate of renal stones. Korean J Urol. 2012; 53:40–43.12. Cleveland RO, Lifshitz DA, Connors BA, Evan AP, Willis LR, Crum LA. In vivo pressure measurements of lithotripsy shock waves in pigs. Ultrasound Med Biol. 1998; 24:293–306.13. Li G, McAteer JA, Williams JC Jr, Berwick ZC. Effect of the body wall on lithotripter shock waves. J Endourol. 2014; 28:446–452.14. Ng CF, Lo AK, Lee KW, Wong KT, Chung WY, Gohel D. A prospective, randomized study of the clinical effects of shock wave delivery for unilateral kidney stones: 60 versus 120 shocks per minute. J Urol. 2012; 188:837–842.15. Hammad FT, Al Najjar A. The effect of fat, muscle, and kidney on stone fragmentation by shockwave lithotripsy: an in vitro study. J Endourol. 2010; 24:289–292.16. Hammad FT, Balakrishnan A. The effect of fat and nonfat components of the skin-to-stone distance on shockwave lithotripsy outcome. J Endourol. 2010; 24:1825–1829.17. Smith SM, Hoy WE, Cobb L. Low incidence of glomerulosclerosis in normal kidneys. Arch Pathol Lab Med. 1989; 113:1253–1255.18. Choudhury D, Levi M. Kidney aging--inevitable or preventable? Nat Rev Nephrol. 2011; 7:706–717.19. Kanasaki K, Kitada M, Koya D. Pathophysiology of the aging kidney and therapeutic interventions. Hypertens Res. 2012; 35:1121–1128.20. Ikegaya H, Kato A, Kumano S, Tominaga T. Correlation between age and the efficacy of ESWL. BJU Int. 2005; 96:1145.21. Ng CF, Wong A, Tolley D. Is extracorporeal shock wave lithotripsy the preferred treatment option for elderly patients with urinary stone? A multivariate analysis of the effect of patient age on treatment outcome. BJU Int. 2007; 100:392–395.22. Jagtap J, Mishra S, Bhattu A, Ganpule A, Sabnis R, Desai M. Evolution of shockwave lithotripsy (SWL) technique: a 25-year single centre experience of >5000 patients. BJU Int. 2014; 114:748–753.23. Ng CF, Thompson TJ, McLornan L, Tolley DA. Single-center experience using three shockwave lithotripters with different generator designs in management of urinary calculi. J Endourol. 2006; 20:1–8.24. Grenier N, Gennisson JL, Cornelis F, Le Bras Y, Couzi L. Renal ultrasound elastography. Diagn Interv Imaging. 2013; 94:545–550.25. Togao O, Doi S, Kuro-o M, Masaki T, Yorioka N, Takahashi M. Assessment of renal fibrosis with diffusion-weighted MR imaging: study with murine model of unilateral ureteral obstruction. Radiology. 2010; 255:772–780.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case Report of Acute Kidney Injury after Extracorporeal Shockwave Lithotripsy
- Extracorporeal shockwave lithotripsy: one year experience with the siemens lithostar
- Extremely-slow, half-number shockwave lithotripsy for asymptomatic renal stones <20 mm
- The Comparison of Efficacy of Ureteroscopic Removal and Shockwave Lithotripsy in Lower Ureteral Stones
- The Effect of Tamsulosin on Expulsion of Ureteral Stones after Extracorporeal Shock Wave Lithotripsy
