Intra-arterial Thrombolysis for Central Retinal Artery Occlusion: Two Cases Report
- Affiliations
-
- 1Department of Neurosurgery, Chuncheon Sacred Heart Hospital, Hallym University, Chuncheon, Korea.
- 2Department of Ophthalmology, Seoul National University Bundang Hospital, Seongnam, Korea.
- 3Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea.
- 4Department of Neurosurgery, Seoul National University Bundang Hospital, Seongnam, Korea. kwonoki@korea.com
- KMID: 2150884
- DOI: http://doi.org/10.3346/jkms.2010.25.6.974
Abstract
- Central retinal artery occlusion (CRAO) causes severe visual loss in affected eye and vision does not recover in more than 90% of the patients. It is believed that it occurs by occlusion of the central retinal artery with small emboli from atherosclerotic plaque of internal cerebral artery. Retina is a part of the brain, thus basically CRAO is corresponding to acute occlusion of intracerebral artery and retinal ischemia is to cerebral stroke. Therefore, intra-arterial thrombolysis (IAT) has been considered as a treatment method in CRAO. Recently, we treated 2 patients diagnosed as CRAO and could achieve complete recanalization on fundus fluorescein angiogram with IAT. Of them, one recovered visual acuity to 20/25. We report our 2 CRAO cases treated with IAT and discuss technical aspects for IAT and management of patient. To the best of our knowledge, this is the first Korean report of IAT for CRAO.
Figure
-
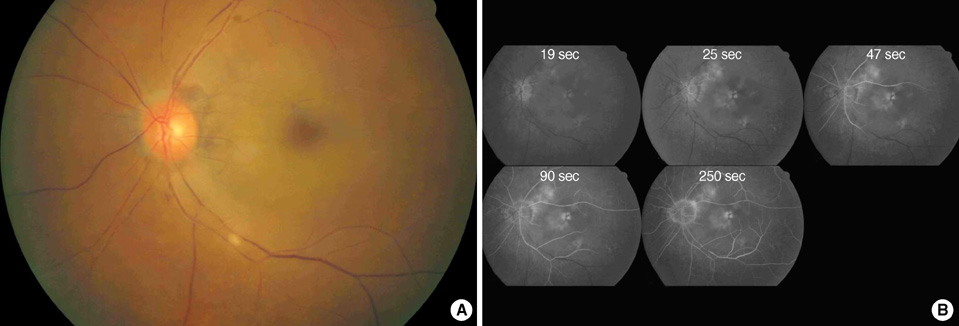
Fig. 1 Fundus photography (A) and fluorescein angiography (B) before intra-arterial thrombolysis in case 1. There was white edematous retina with typical cherry-red spot and fragmentation of retinal vessels compatible with central retinal artery occlustion (A). Retinal arterial filling was markedly delayed with arterio-venous transit time of 5 min. The choroidal perfusion was normal (B).
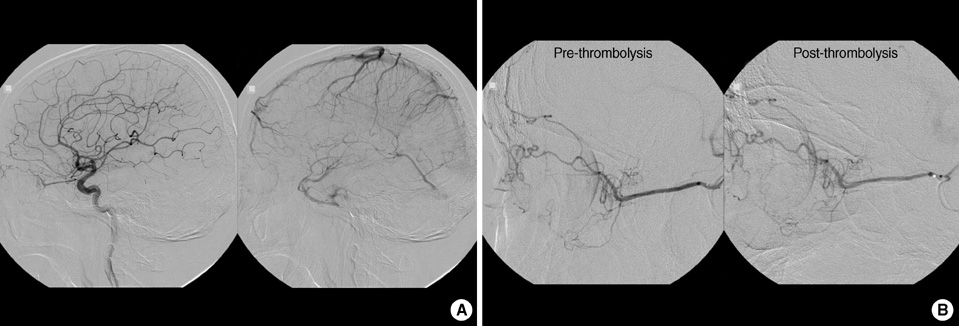
Fig. 2 Arterial phase and venous phase of left internal carotid angiogram (A) in case 1. Ophthalmic artery and chroidal blush were observed. Selective angiogram before and after intra-arterial thrombolysis (B). There was no definite occlusion in ciliary arteries and other muscular branches from ophthalmic artery. Intra-arterial thrombolysis was performed with urokinase and abxicimab.
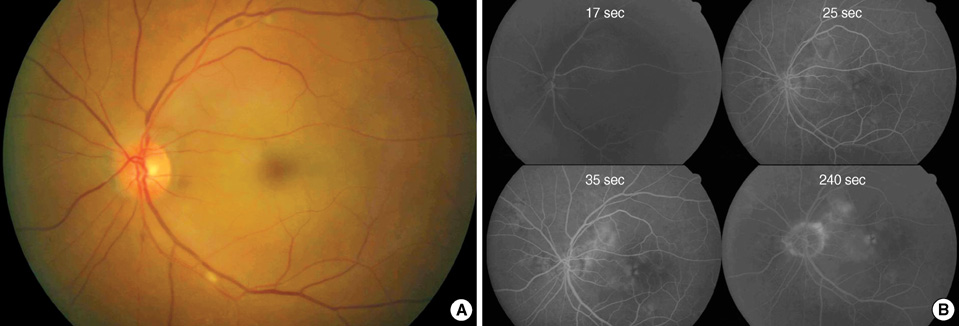
Fig. 3 Fundus photography (A) and fluorescein angiography (B). One day after intra-arterial thrombolysis in case 1. Perfusion of retinal vessels were normalized and retinal color was restored to normal orange hue. However, there still remained macular edema (A). Retinal arterial and venous filling was normalized with arterio-venous transit time was 18 sec (B).
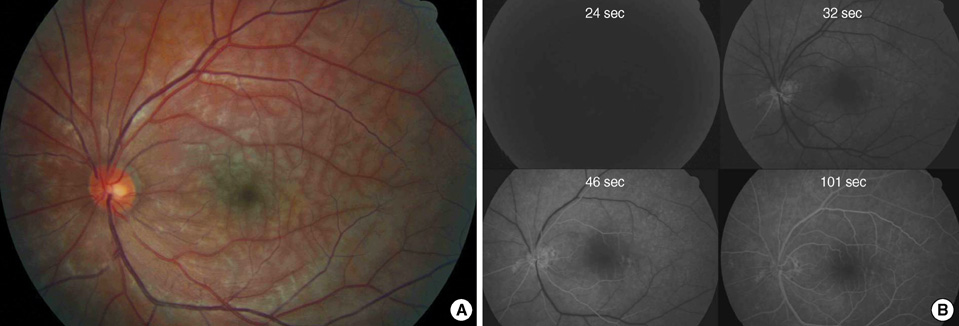
Fig. 4 Fundus photogrphy (A) and fluorescein angiography (B) before intra-arterial thrombolysis in case 2. There is diffuse ischemic retinal edema throughout the entire fundus (A). The visual acuity was 20/70. There is delay in arterial filling and the arteriovenous transit time is 70 sec (B).
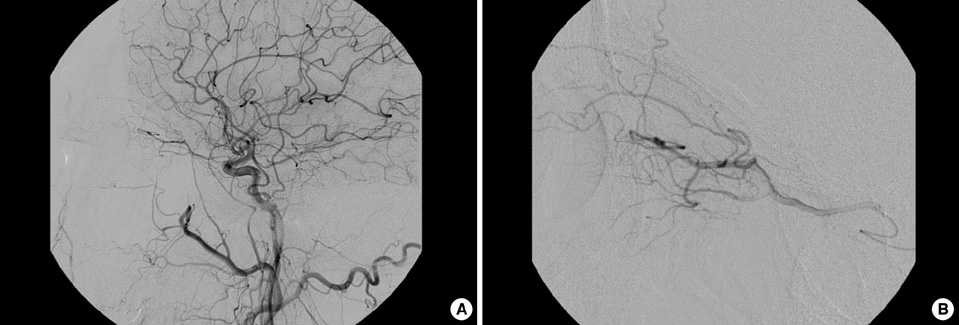
Fig. 5 Common carotid angiogram in case 2 (A). There was no definite occlusion and remarkable lesion in ophthalmic artery and main trunk of intracerebral arteries. Selective angiogram of ophthalmic artery after intra-arterial thrombolysis (B). The muscular branches and ciliary arteries were well shown.
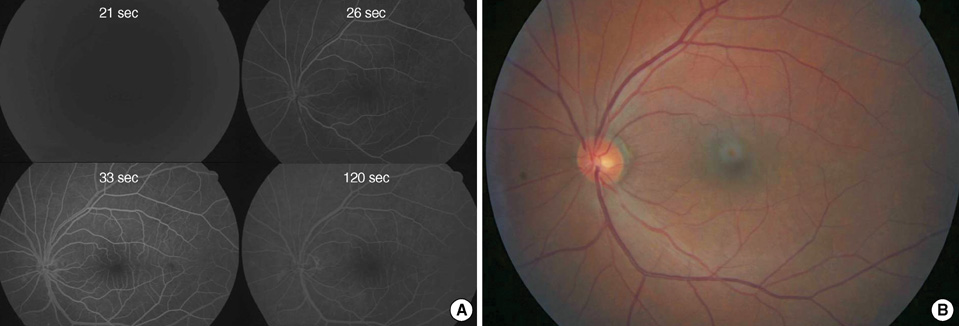
Fig. 6 Fluorescein angiography 1day after intra-arterial thrombolysis in case 2 (A). The retinal perfusion restored to normal and arteriovenous transit time is 12 sec. Fundus photography 2 weeks after thrombolysis (B). There is no more retinal edema suggesting previous ischemia. The vision improved to 20/25.
Reference
-
1. Hayreh SS, Zimmerman MB. Central retinal artery occlusion: visual outcome. Am J Ophthalmol. 2005. 140:376–391.2. Rumelt S, Dorenboim Y, Rehany U. Aggressive systematic treatment for central retinal artery occlusion. Am J Ophthalmol. 1999. 128:733–738.3. Atebara NH, Brown GC, Cater J. Efficacy of anterior chamber paracentesis and Carbogen in treating acute nonarteritic central retinal artery occlusion. Ophthalmology. 1995. 102:2029–2034.4. Mueller AJ, Neubauer AS, Schaller U, Kampik A. Evaluation of minimally invasive therapies and rationale for a prospective randomized trial to evaluate selective intra-arterial lysis for clinically complete central retinal artery occlusion. Arch Ophthalmol. 2003. 121:1377–1381.5. Arnold M, Koerner U, Remonda L, Nedeltchev K, Mattle HP, Schroth G, Sturzenegger M, Weber J, Koerner F. Comparison of intra-arterial thrombolysis with conventional treatment in patients with acute central retinal artery occlusion. J Neurol Neurosurg Psychiatry. 2005. 76:196–199.6. Beatty S, Au Eong KG. Local intra-arterial fibrinolysis for acute occlusion of the central retinal artery: a meta-analysis of the published data. Br J Ophthalmol. 2000. 84:914–916.7. Butz B, Strotzer M, Manke C, Roider J, Link J, Lenhart M. Selective intraarterial fibrinolysis of acute central retinal artery occlusion. Acta Radiol. 2003. 44:680–684.8. Framme C, Spiegel D, Roider J, Sachs HG, Lohmann CP, Butz B, Link J, Gabel VP. Central retinal artery occlusion. Importance of selective intra-arterial fibrinolysis. Ophthalmologe. 2001. 98:725–730.9. Kattah JC, Wang DZ, Reddy C. Intravenous recombinant tissue-type plasminogen activator thrombolysis in treatment of central retinal artery occlusion. Arch Ophthalmol. 2002. 120:1234–1236.10. Schmidt DP, Schulte-Monting J, Schumacher M. Prognosis of central retinal artery occlusion: local intraarterial fibrinolysis versus conservative treatment. AJNR Am J Neuroradiol. 2002. 23:1301–1307.11. Noble J, Weizblit N, Baerlocher MO, Eng KT. Intra-arterial thrombolysis for central retinal artery occlusion: a systematic review. Br J Ophthalmol. 2008. 92:588–593.12. Plant GT, Landau K. Thrombolysis for central retinal artery occlusion. J Neurol Neurosurg Psychiatry. 2005. 76:160–161.13. Hayreh SS. Retinal arterial occlusion with LIF using rTPA. Ophthalmology. 1999. 106:1236–1239.14. Schumacher M, Schmidt D, Wakhloo AK. Intra-arterial fibrinolytic therapy in central retinal artery occlusion. Neuroradiology. 1993. 35:600–605.15. Rumelt S, Brown GC. Update on treatment of retinal arterial occlusions. Curr Opin Ophthalmol. 2003. 14:139–141.16. Biousse V, Calvetti O, Bruce BB, Newman NJ. Thrombolysis for central retinal artery occlusion. J Neuroophthalmol. 2007. 27:215–230.17. Benavente O, Eliasziw M, Streifler JY, Fox AJ, Barnett HJ, Meldrum H. Prognosis after transient monocular blindness associated with carotid-artery stenosis. N Engl J Med. 2001. 345:1084–1090.18. Streifler JY, Eliasziw M, Benavente OR, Harbison JW, Hachinski VC, Barnett HJ, Simard D. The risk of stroke in patients with first-ever retinal vs hemispheric transient ischemic attacks and high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial. Arch Neurol. 1995. 52:246–249.19. Biousse V, Trobe JD. Transient monocular visual loss. Am J Ophthalmol. 2005. 140:717–721.20. Feltgen N, Neubauer A, Jurklies B, Schmoor C, Schmidt D, Wanke J, Maier-Lenz H, Schumacher M. Multicenter study of the European Assessment Group for Lysis in the Eye (EAGLE) for the treatment of central retinal artery occlusion: design issues and implications. EAGLE Study report no. 1: EAGLE Study report no. 1. Graefes Arch Clin Exp Ophthalmol. 2006. 244:950–956.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intra-arterial Thrombolysis for Central Retinal Artery Occlusion after the Coil Embolization of Paraclinoid Aneurysm
- The Effect of Intra-arterial Thrombolysis in Retinal Artery Occlusion: Case Series and Literature Review
- Favorable outcome after intra-arterial thrombolysis in a patient with branch retinal artery occlusion: a case report
- A Clinical Study of 36 Cases of Retinal Artery Occlusion
- Incomplete Central Retinal Artery Occlusion
