Hip Pelvis.
2015 Dec;27(4):241-249. 10.5371/hp.2015.27.4.241.
Open Surgical Treatment for Femoroacetabular Impingement in Patients over Thirty Years: Two Years Follow-up Results
- Affiliations
-
- 1Department of Orthopaedic Surgery, Changwon Hospital, Changwon, Korea. suhyun1123@naver.com
- KMID: 2150512
- DOI: http://doi.org/10.5371/hp.2015.27.4.241
Abstract
- PURPOSE
We report short term results of open surgical treatment for symptomatic femoroacetabular impingement (FAI) in patients over the age of 30 years.
MATERIALS AND METHODS
Between May 2011 and June 2012, thirteen FAI hips (11 patients) with hip pain persisting longer than 6 months were treated by either surgical hip dislocation (SHD) or anterior mini-open. They were followed up for longer than 2 years. The 11 patients included 7 females and 4 males with a mean age of 45 (range, 33-60) years. They were clinically evaluated for modified Harris hip score (MHHS) and University of California at Los Angeles (UCLA) activity level. Their lateral center-edge angle, acetabular index, and alpha angle were measured and compared.
RESULTS
Acetabuloplasties were performed for seven cases. Femoral osteochondroplasty was performed for all thirteen cases. At minimum follow-up of two year (range, 24-29 months), all patients had substantial relief in preoperative pain with improvement in range of motion. The median MHHS was significantly (P<0.05) improved from 61 points preoperatively to 87 points at the last follow-up. The median UCLA activity level was 7 (range, 5-8) at last follow-up. Radiological indices improved. Two cases showed mild residual pain attributable to adhesion between capsule and reshaped femoral head-neck area.
CONCLUSION
Open surgical treatment of FAI was a reliable and effective treatment method in symptomatic FAIs for patients over the age of 30 years without advanced arthritic change of hip joint at short term follow-up.
Keyword
MeSH Terms
Figure
-

Fig. 1 Bony bump of anterior femoral head-neck junction removed by anterior mini-open.
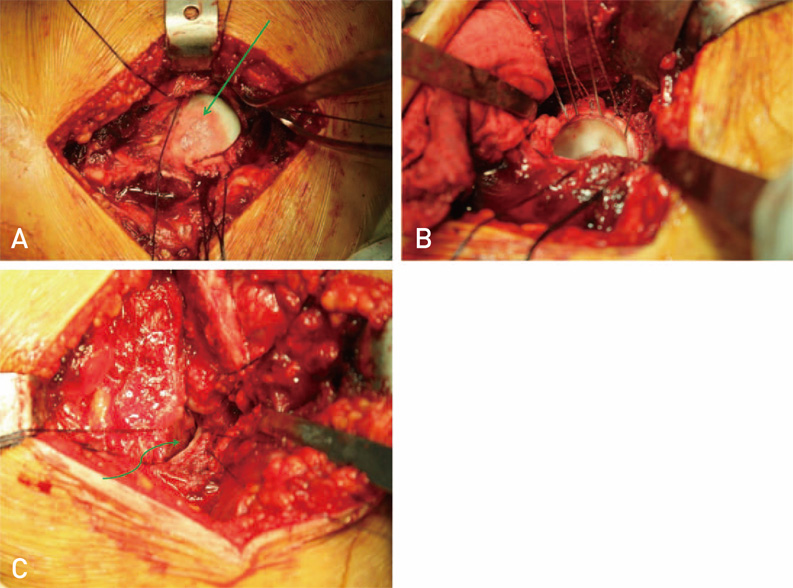
Fig. 2 (A) Periosteal blushing (arrow) in head neck junction. (B) Labral takedown, rim resection and labral refixation by surgical hip dislocation. (C) Clearance of impingement (arrow) after femoral osteochondroplasty.

Fig. 3 Change of lateral center-edge angle. (A) 50° before acetabular osteochondroplasty; (B) 36° after acetabular osteochondroplasty. (C) The arrow indicates area of trimmed acetabular rim on computed tomogram.

Fig. 4 Shape of femoral head-neck junction. (A) Before femoral osteochondroplasty. (B) After femoral osteochondroplasty.
Reference
-
1. Lavigne M, Parvizi J, Beck M, Siebenrock KA, Ganz R, Leunig M. Anterior femoroacetabular impingement: part I. Techniques of joint preserving surgery. Clin Orthop Relat Res. 2004; (418):61–66.2. Ganz R, Gill TJ, Gautier E, Ganz K, Krügel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001; 83:1119–1124.3. Cohen SB, Huang R, Ciccotti MG, Dodson CC, Parvizi J. Treatment of femoroacetabular impingement in athletes using a mini-direct anterior approach. Am J Sports Med. 2012; 40:1620–1627.
Article4. Parvizi J, Huang R, Diaz-Ledezma C, Og B. Mini-open femoroacetabular osteoplasty: how do these patients do? J Arthroplasty. 2012; 27:8 Suppl. 122–125.e1.5. Boone GR, Pagnotto MR, Walker JA, Trousdale RT, Sierra RJ. Caution should be taken in performing surgical hip dislocation for the treatment of femoroacetabular impingement in patients over the age of 40. HSS J. 2012; 8:230–234.
Article6. Tannast M, Siebenrock KA, Anderson SE. Femoroacetabular impingement: radiographic diagnosis--what the radiologist should know. AJR Am J Roentgenol. 2007; 188:1540–1552.
Article7. Kalberer F, Sierra RJ, Madan SS, Ganz R, Leunig M. Ischial spine projection into the pelvis : a new sign for acetabular retroversion. Clin Orthop Relat Res. 2008; 466:677–683.8. Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002; 84:556–560.
Article9. Clohisy JC, Carlisle JC, Beaulé PE, et al. A systematic approach to the plain radiographic evaluation of the young adult hip. J Bone Joint Surg Am. 2008; 90:Suppl 4. 47–66.
Article10. Harris MD, Kapron AL, Peters CL, Anderson AE. Correlations between the alpha angle and femoral head asphericity: Implications and recommendations for the diagnosis of cam femoroacetabular impingement. Eur J Radiol. 2014; 83:788–796.
Article11. Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003; (417):112–120.12. Tannast M, Siebenrock KA. Open therapy of femoroacetabular impingement. Oper Orthop Traumatol. 2010; 22:3–16.13. Peters CL, Schabel K, Anderson L, Erickson J. Open treatment of femoroacetabular impingement is associated with clinical improvement and low complication rate at short-term followup. Clin Orthop Relat Res. 2010; 468:504–510.
Article14. Steppacher SD, Huemmer C, Schwab JM, Tannast M, Siebenrock KA. Surgical hip dislocation for treatment of femoroacetabular impingement: factors predicting 5-year survivorship. Clin Orthop Relat Res. 2014; 472:337–348.
Article15. Bedi A, Chen N, Robertson W, Kelly BT. The management of labral tears and femoroacetabular impingement of the hip in the young, active patient. Arthroscopy. 2008; 24:1135–1145.
Article16. Ferguson SJ, Bryant JT, Ganz R, Ito K. The acetabular labrum seal: a poroelastic finite element model. Clin Biomech (Bristol, Avo). 2000; 15:463–468.
Article17. Kim YT, Azuma H. The nerve endings of the acetabular labrum. Clin Orthop Relat Res. 1995; (320):176–181.
Article18. Espinosa N, Rothenfluh DA, Beck M, Ganz R, Leunig M. Treatment of femoro-acetabular impingement: preliminary results of labral refixation. J Bone Joint Surg Am. 2006; 88:925–935.19. Walker JA, Pagnotto M, Trousdale RT, Sierra RJ. Preliminary pain and function after labral reconstruction during femoroacetabular impingement surgery. Clin Orthop Relat Res. 2012; 470:3414–3420.
Article20. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005; 87:1012–1018.21. Anderson LA, Peters CL, Park BB, Stoddard GJ, Erickson JA, Crim JR. Acetabular cartilage delamination in femoroacetabular impingement. Risk factors and magnetic resonance imaging diagnosis. J Bone Joint Surg Am. 2009; 91:305–313.22. Peters CL, Stronach BM, Pelt CE, Erickson JA. Open surgical dislocation for the treatment of femoroacetabular impingement: past, present, and future. Instr Course Lect. 2012; 61:273–286.23. Naal FD, Miozzari HH, Schär M, Hesper T, Nötzli HP. Midterm results of surgical hip dislocation for the treatment of femoroacetabular impingement. Am J Sports Med. 2012; 40:1501–1510.
Article24. Yun HH, Shon WY, Yun JY. Treatment of femoroacetabular impingement with surgical dislocation. Clin Orthop Surg. 2009; 1:146–154.
Article25. Beaulé PE, Le Duff MJ, Zaragoza E. Quality of life following femoral head-neck osteochondroplasty for femoroacetabular impingement. J Bone Joint Surg Am. 2007; 89:773–779.
Article26. Krueger A, Leunig M, Siebenrock KA, Beck M. Hip arthroscopy after previous surgical hip dislocation for femoroacetabular impingement. Arthroscopy. 2007; 23:1285–1289.e1.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Arthroscopic Treatment of Femoroacetabular Impingement of the Hip: 5-7 Years Result
- Controversial Issues in Arthroscopic Surgery for Femoroacetabular Impingement
- Acetabular Labral Tears in Patients with Sports Injury
- Arthroscopic Labral Repair Associated with Femoroacetabular Impingement: Short Term 2-5 Years Follow-up Results
- Efficacy of Intra-articular Steroid Injection in Patients with Femoroacetabular Impingement
