Tumoral Calcinosis of the Index Finger: A Case Report
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Bundang Jesaeng Hospital, Seongnam, Korea. kty@dmc.or.kr
- 2Department of Pathology, Bundang Jesaeng Hospital, Seongnam, Korea.
- KMID: 2150402
- DOI: http://doi.org/10.12790/jkssh.2015.20.4.193
Abstract
- Tumoral calcinosis is a type of idiopathic calcinosis cutis which usually occurs around the large joints due to deposition of calcium phosphate, but extremely rare in the fingers which has been reported less than 20 cases in the literature. When it occurs on the fingers, it shows almost normal skin appearance and no specific symptoms except localized tenderness and numbness, therefore it is difficult to differential diagnosis among other common tumors on the fingers. In most cases surgical excision is performed before final diagnosis, and it is easy to misdiagnosis. The patient had mass like lesion which is enlarging for last 2 years at the radial side of the second finger without any trauma history. We prediagnosed the tumoral calcinosis with the simple radiologic test and laboratory tests and performed surgical excision without recurrence. So we report a case of tumoral calcinosis of the radial side of the second finger with brief review of the literature.
Keyword
MeSH Terms
Figure
-
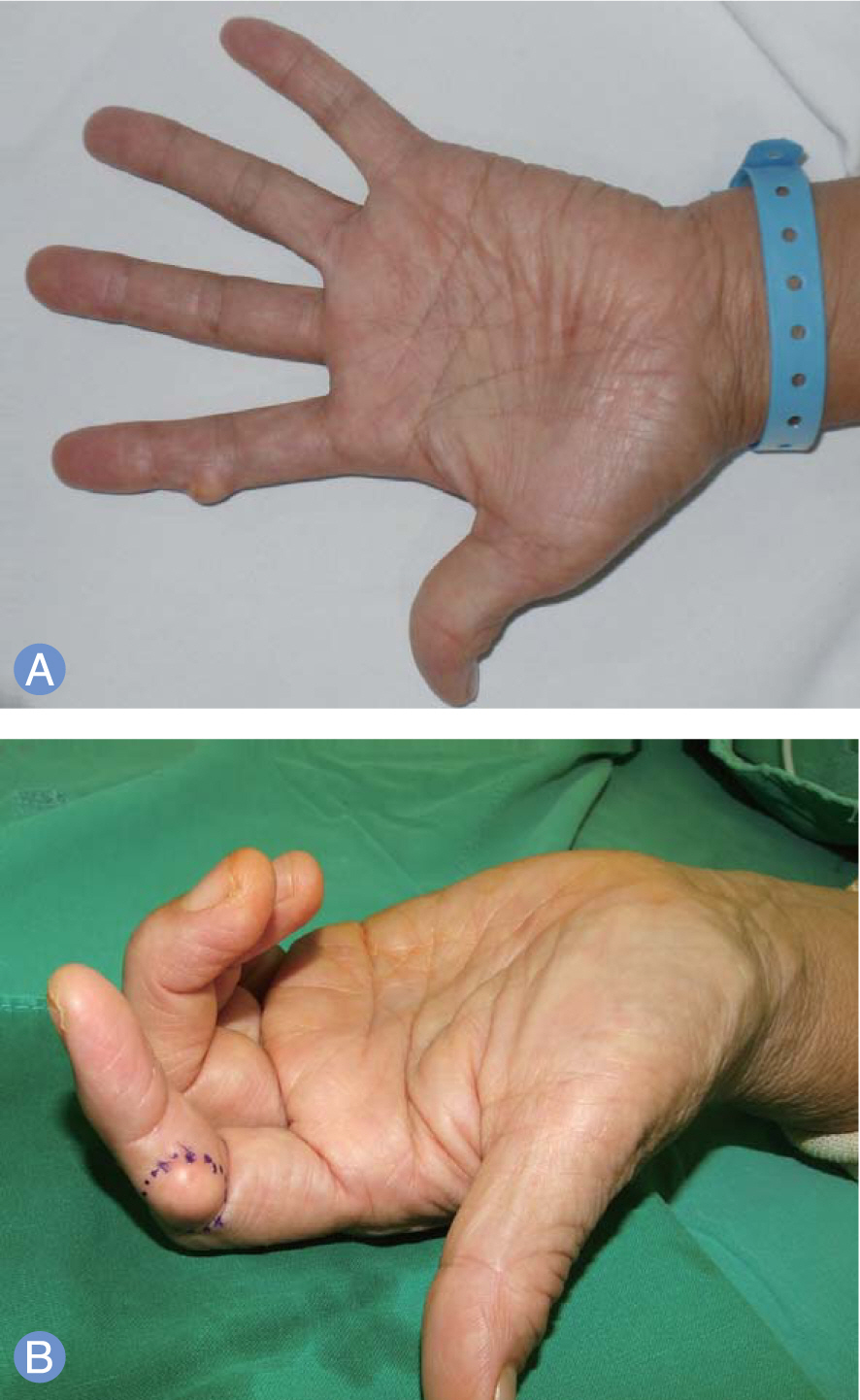
Fig. 1. (A, B) Preoperative appearance of the lesion at the radial side of the proximal interphalangeal joint of left index finger. There was paresthesia on the ipsilateral distal area of the tumor and physical examination revealed a firm, round and tender mass.

Fig. 2. Standard radiographs showed a well-demarcated, oval-shaped, densely opacified mass on the proximal interphalangeal joint of the left index finger. (A) Antero-posteriorview. (B) Oblique view.
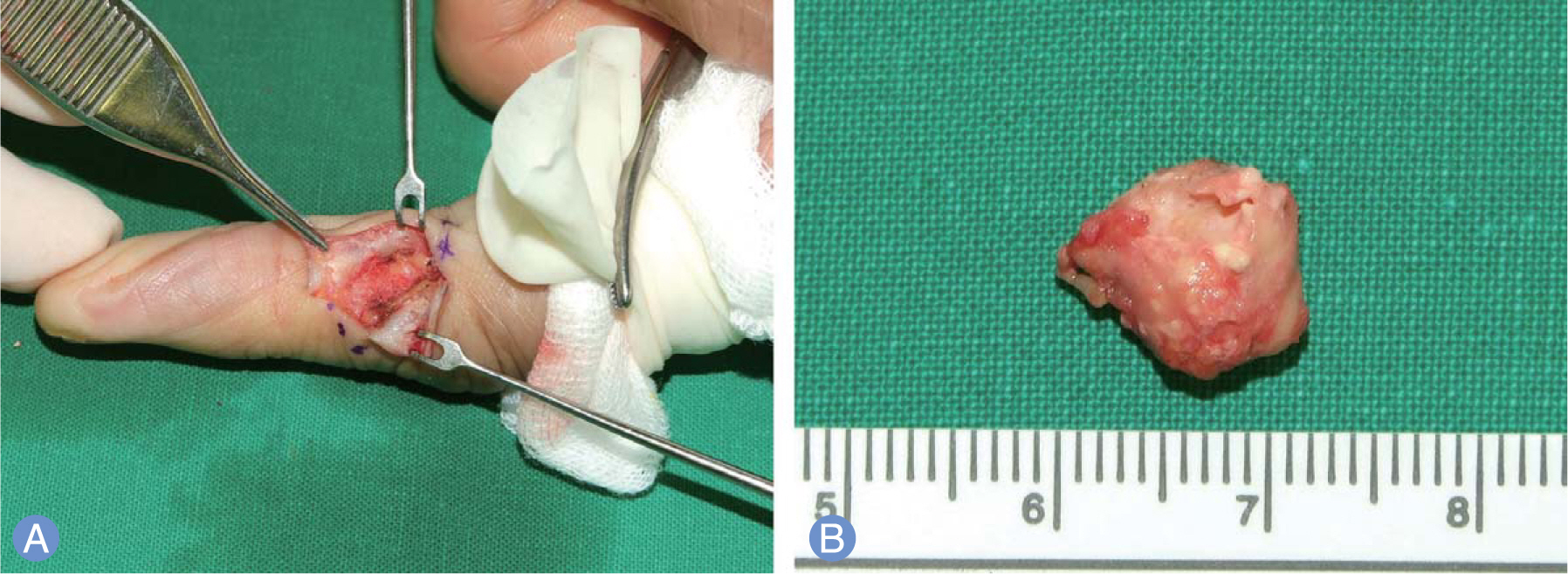
Fig. 3. (A) Intraoperative findings. Yellowish thin capsulated calcified mass with irregular surface was located on subcutaneous level without adhesion to surrounding tissue, and well demarcated. (B) The size of the mass was 12×11 mm. The yellow capsule con-tainedchalkyfluid.
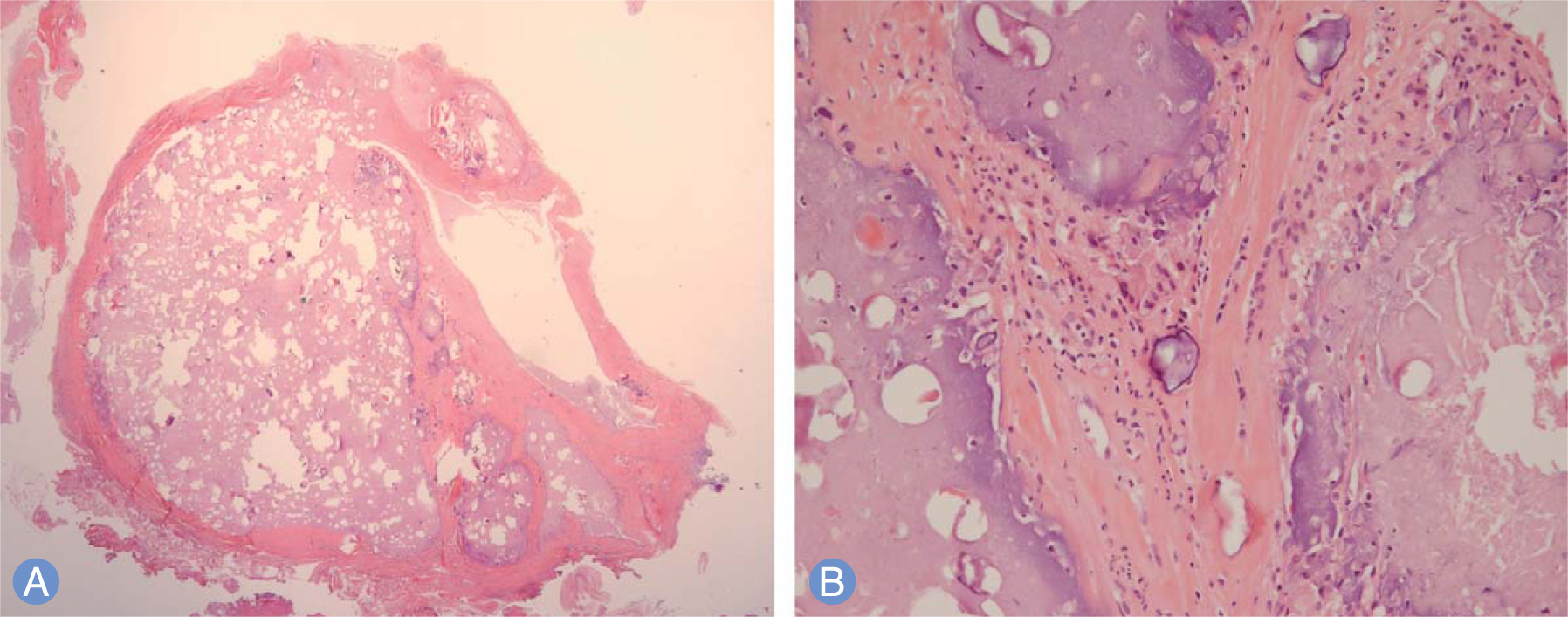
Fig. 4. (A) The mass consisted of calcified material and fibrous tissue (H&E, ×10). (B) Fibrous tissue and multi-nucleated giant cells appeared around the calcified material (H&E, ×200).
Reference
-
References
1. Mitnick PD, Goldfarb S, Slatopolsky E, Lemann J Jr, Gray RW, Agus ZS. Calcium and phosphate metabolism in tumoral calcinosis. Ann Intern Med. 1980; 92:482–7.
Article2. Inclan A, Leon PP, Camejo M, Tumoral calcinosis JAMA. 1943; 121:490–5.3. Murai S, Matsui M, Nakamura A. Tumoral calcinosis in both index fingers: a case report. Scand J Plast Reconstr Surg Hand Surg. 2001; 35:433–5.4. Smack D, Norton SA, Fitzpatrick JE. Proposal for a pathogenesis-based classification of tumoral calcinosis. Int J Dermatol. 1996; 35:265–71.
Article5. Topaz O, Shurman DL, Bergman R, et al. Mutations in GALNT3, encoding a protein involved in O-linked glycosylation, cause familial tumoral calcinosis. Nat Genet. 2004; 36:579–81.
Article6. Olsen KM, Chew FS. Tumoral calcinosis: pearls, polemics, and alternative possibilities. Radiographics. 2006; 26:871–85.
Article7. Nikci V, Doumas C. Calcium deposits in the hand and wrist. J Am Acad Orthop Surg. 2015; 23:87–94.
Article8. Martinez S, Vogler JB 3rd, Harrelson JM, Lyles KW. Imaging of tumoral calcinosis: new observations. Radiology. 1990; 174:215–22.
Article9. Hug I, Guncaga J. Tumoral calcinosis with sedimentation sign. Br J Radiol. 1974; 47:734–6.
Article10. Sebesta A, Kamineni S, Dumont CE. Idiopathic tumoral calcinosis of the index finger: case report. Scand J Plast Reconstr Surg Hand Surg. 2000; 34:405–8.
