Modified Split Ulnar Gutter Splint for Treatment of Fifth Metacarpal Neck Fractures
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. ygchung@catholic.ac.kr
- KMID: 2150397
- DOI: http://doi.org/10.12790/jkssh.2015.20.4.161
Abstract
- PURPOSE
To evaluate radiological results of the modified split ulnar gutter splint for the fifth metacarpal neck fracture.
METHODS
Between December 2008 and May 2014, 17 patients (18 cases) with fifth metacarpal neck fractures were managed with our modified split ulnar gutter splint. Radiological outcomes in oblique and lateral radiographs were evaluated. Mean immobilization period was 4.9 weeks (range, 4-7) weeks. Mean follow-up period was 17.1 week (range, 8-80 weeks).
RESULTS
All of 18 fractures were completely united. The average of prereduction dorsal angulation, 27degrees in the oblique radiographs and 21degrees in the lateral radiographs, were corrected to 17degrees in the oblique radiographs and 10degrees in the lateral radiographs after closed reduction. At the last follow-up, they were 14degrees and 11degrees respectively. The mean difference of angulation deformity between in postreduction and final follow-up radiograms were 3degrees in the oblique radiographs and 1degrees in the lateral radiographs, which was not significantly different.
CONCLUSION
Immobilization using modified split ulnar gutter splint will be a reliable option for the fifth metacarpal neck fractures in selected patients, which will avoid the surgeries.
Figure
-
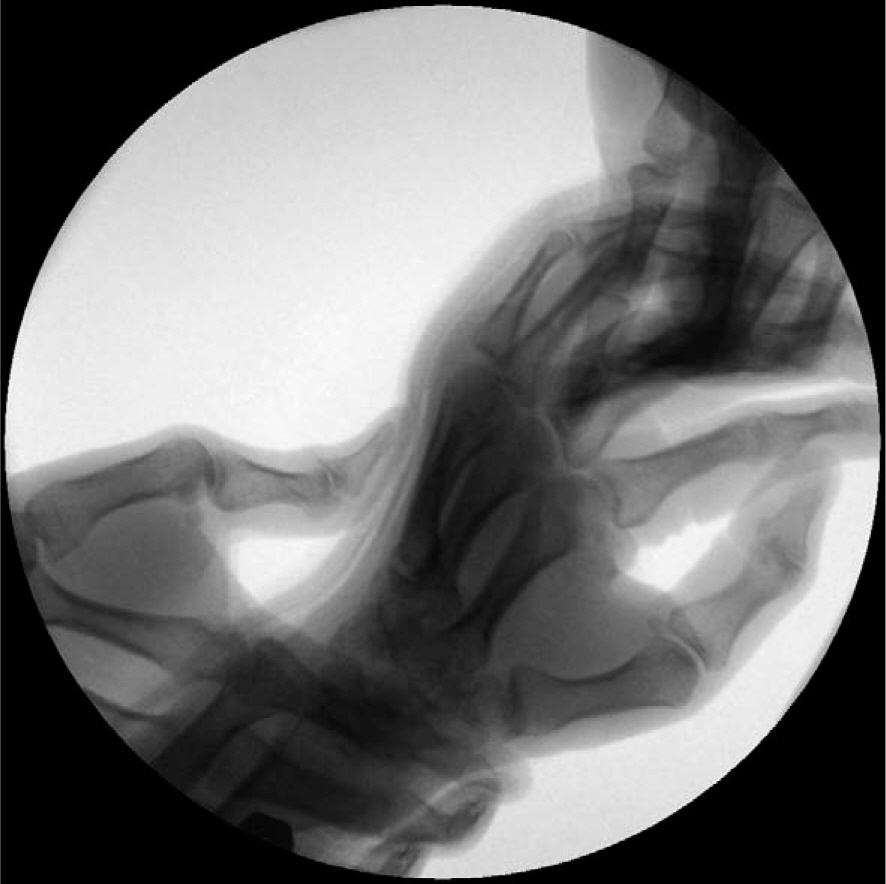
Fig. 1. Reduction method under image intensifier. Longitudinal traction applied while proximal phalanx was elevated toward dorsal direction and metacarpal shaft put down.

Fig. 2. Molding method of modified split ulnar gutter splint.

Fig. 3. (A) A 50-year-old man sustained a fifth metacarpal neck fracture with 24.5° angulation deformity on oblique radiograph, 18° angulation on lateral radiograph. (B) Post-reduction radiographs show 14.4°, 9° residual angulation on oblique and lateral radiographs, respectively. (C) 24-month follow-up radiographs show good union without any reduction loss or rotationalde deformity.
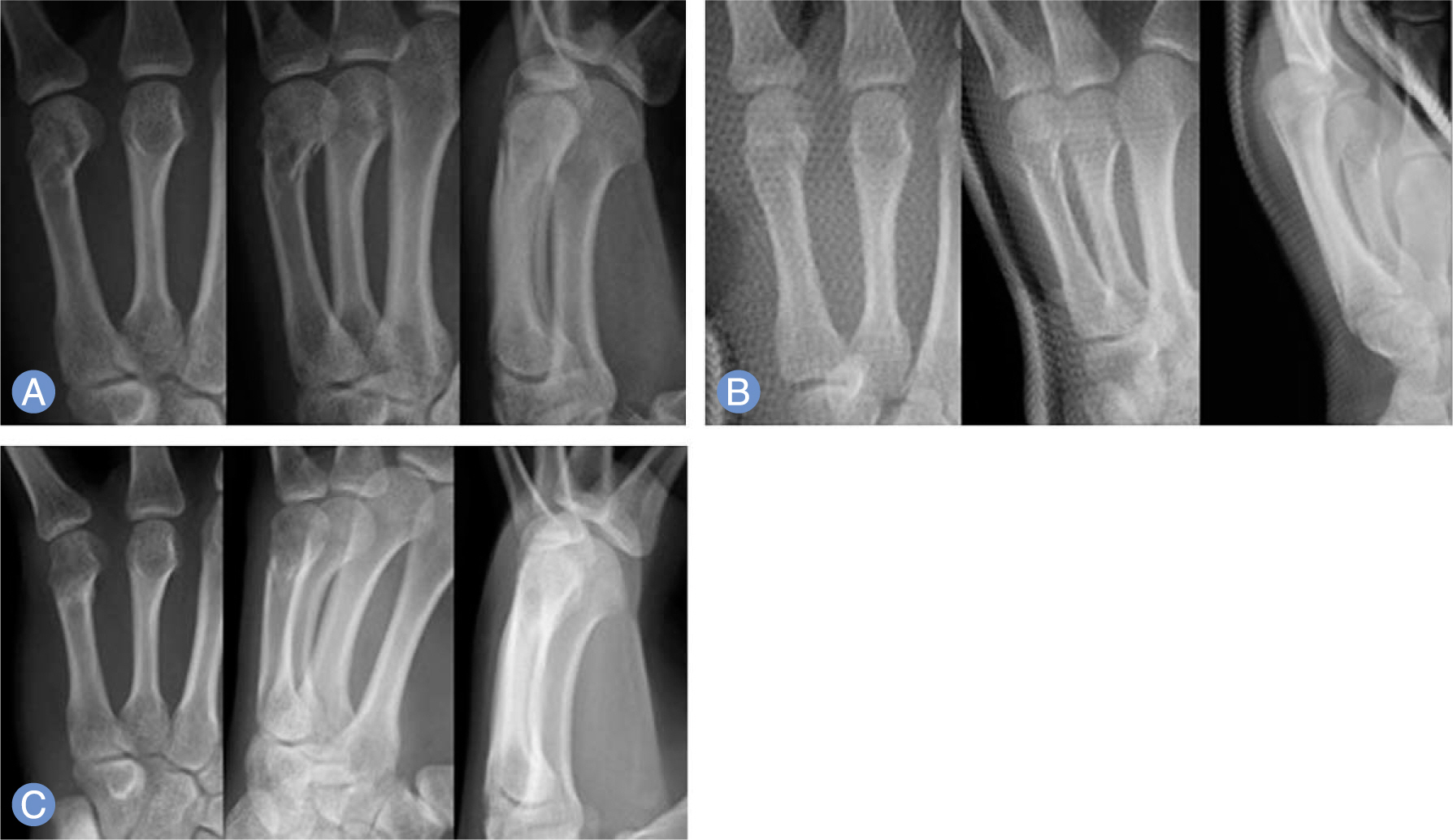
Fig. 4. (A) A 28-year-old man sustained a fifth metacarpal neck fracture with 16.5° angulation deformity on oblique radiograph, 6° angulation on lateral radiograph. (B) Post-reduction radiographs show 1.6°, 2° residual angulation on oblique and lateral radiographs, respectively. (C) 10-week follow-up radiographs show good union and 2.3°, 2° angulation on oblique and lateral radiographs, respectively.
Cited by 1 articles
-
Management of metacarpal and phalangeal fractures
Seungbum Chae, Il-Jung Park
Arch Hand Microsurg. 2023;28(2):75-86. doi: 10.12790/ahm.23.0005.
Reference
-
References
1. Hunter JM, Cowen NJ. Fifth metacarpal fractures in a compensation clinic population: a report on one hundred and thirty-three cases. J Bone Joint Surg Am. 1970; 52:1159–65.2. McCue FC 3rd, Meister K. Common sports hand injuries: an overview of aetiology, management and prevention. Sports Med. 1993; 15:281–9.3. Ford DJ, Ali MS, Steel WM. Fractures of the fifth metacarpal neck: is reduction or immobilisation necessary? J Hand Surg Br. 1989; 14:165–7.
Article4. Theeuwen GA, Lemmens JA. van Niekerk JL. Conservative treatment of boxer's fracture: a retrospective analysis. Injury. 1991; 22:394–6.5. Ali A, Hamman J, Mass DP. The biomechanical effects of angulated boxer's fractures. J Hand Surg Am. 1999; 24:835–44.
Article6. Birndorf MS, Daley R, Greenwald DP. Metacarpal fracture angulation decreases flexor mechanical efficiency in human hands. Plast Reconstr Surg. 1997; 99:1079–83.
Article7. Braakman M, Oderwald EE, Haentjens MH. Functional taping of fractures of the 5th metacarpal results in a quicker recovery. Injury. 1998; 29:5–9.
Article8. Lowdon IM. Fractures of the metacarpal neck of the little finger. Injury. 1986; 17:189–92.
Article9. Maitra A, Sen B. Displaced boxers' fractures: a simple and effective method of external splintage. Br J Clin Pract. 1990; 44:348–51.10. McKerrell J, Bowen V, Johnston G, Zondervan J. Boxer's fractures: conservative or operative management? J Trauma. 1987; 27:486–90.11. Porter ML, Hodgkinson JP, Hirst P, Wharton MR, Cunliffe M. The boxers' fracture: a prospective study of functional recovery. Arch Emerg Med. 1988; 5:212–5.
Article12. Jahss SA. Fractures of the metacarpals. J Bone Joint Surg Am. 1938; 20:178–86.13. Pace GI, Gendelberg D, Taylor KF. The effect of closed reduction of small finger metacarpal neck fractures on the ultimate angular deformity. J Hand Surg Am. 2015; 40:1582–5.
Article14. Leung YL, Beredjiklian PK, Monaghan BA, Bozentka DJ. Radiographic assessment of small finger metacarpal neck fractures. J Hand Surg Am. 2002; 27:443–8.
Article15. Foucher G. "Bouquet" osteosynthesis in metacarpal neck fractures: a series of 66 patients. J Hand Surg Am. 1995; 20:S86–90.
Article16. Lane CS, Kennedy JF, Kuschner SH. The reverse oblique x-ray film: metacarpal fractures revealed. J Hand Surg Am. 1992; 17:504–6.
Article17. Bloem JJ. The treatment and prognosis of uncomplicated dislocated fractures of the metacarpals and phalanges. Arch Chir Neerl. 1971; 23:55–65.
Article18. Kang HJ, Song KW, Park KK, Sung SY, Hahn SB. Comparison between operative and conservative treatment of the 5th metacarpal neck fracture. J Korean Orthop Assoc. 2004; 39:203–9.
Article19. Harding IJ, Parry D, Barrington RL. The use of a moulded metacarpal brace versus neighbour strapping for fractures of the little finger metacarpal neck. J Hand Surg Br. 2001; 26:261–3.
Article20. Kuokkanen HO, Mulari-Keranen SK, Niskanen RO, Haapala JK, Korkala OL. Treatment of subcapital fractures of the fifth metacarpal bone: a prospective randomised comparison between functional treatment and reposition and splinting. Scand J Plast Reconstr Surg Hand Surg. 1999; 33:315–7.21. Statius Muller MG, Poolman RW, van Hoogstraten MJ, Steller EP. Immediate mobilization gives good results in boxer's fractures with volar angulation up to 70 degrees: a prospective randomized trial comparing immediate mobilization with cast immobilization. Arch Orthop Trauma Surg. 2003; 123:534–7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Comparison of Sugar Tong Splint and Radial Gutter Short Arm Splint after Closed Reduction of Distal Radius Fracture
- Computed tomography-based analysis of the characteristics of fifth metacarpal neck fractures and its clinical applications
- Open reduction and internal fixation of metacarpal fractures using a thermoplastic splint as a surgical instrument
- Clinical Outcomes of Customized Staple Fixation Using K-wire in Metacarpal Base or Neck Fractures
- Antegrade Intramedullary Prebent K-wire Fixation for the 5th Metacarpal Neck Fracture
