Failure of Flow Diverter Treatment of Intracranial Aneurysms Related to the Fetal-type Posterior Communicating Artery
- Affiliations
-
- 1Division of Neurosurgery, Department of Surgery, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Queen Mary Hospital, Hong Kong. acotsang@hku.hk
- 2Department of Radiology, Queen Mary Hospital, Hong Kong.
- KMID: 2148995
- DOI: http://doi.org/10.5469/neuroint.2015.10.2.60
Abstract
- PURPOSE
The pipeline embolization device (PED) is a flow diverter that has shown promise in the treatment of intracranial aneurysms. Close to one-fifth of aneurysms, however, fail to occlude after PED placement. This study aims to identify anatomical features and clinicopathologic factors that may predispose failed aneurysm occlusion with the PED.
MATERIALS AND METHODS
We retrospectively reviewed all anterior circulation unruptured saccular aneurysms treated with the PED in a single-center. The primary outcome measure was angiographic occlusion. Anatomical features and potential predictors, including gender, aneurysm location, size, height, aspect ratio, neck width, prior treatment and the number of PED, were studied using binary logistic regression.
RESULTS
29 anterior circulation unruptured saccular aneurysms with a mean size of 6.99 mm treated with the PED in a single center were retrospectively studied. The overall occlusion rate was 79.3% after a mean follow-up of 9.2 months. Four aneurysms were related to the fetal-type posterior communicating artery (PComA), and all were refractory to flow diverter treatment. Female gender was significantly associated with a higher occlusion rate. We present the anatomical features and propose possible pathophysiological mechanisms of these PComA aneurysms that failed flow diverter treatment.
CONCLUSION
A PComA aneurysm with persistent fetal-type circulation appears to be particularly refractory to flow diverter treatment, especially when the aneurysm incorporates a significant portion of the PComA. Our experience suggested that flow diverting stents alone may not be the ideal treatment for this subgroup of aneurysms, and alternative modalities should be considered. Female patients were found to have a significantly higher rate of treatment success.
Keyword
MeSH Terms
Figure
-
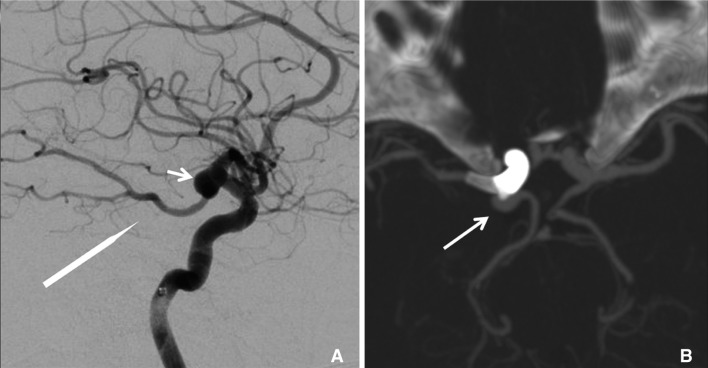
Fig. 1 Patient 1. (A) Pre-treatment digital subtraction angiography showing the fetal-type posterior communicating artery circulation (long arrow) and aneurysm (arrow); (B) curve reformation of the post-treatment CTA showed that the right PComA IA was receiving persistent supply from the fetal PComA (arrow).
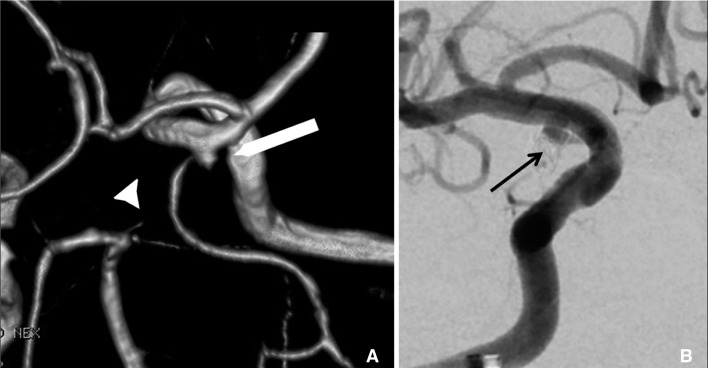
Fig. 2 Patient 2.(A) Pre-treatment computer tomography angiography showing the right posterior communicating artery (PComA) aneurysm remnant (long arrow), which was previously treated with four GDC coils, and the atrophic right P1 segment (arrowhead) associated with fetal-type; (B) control DSA showing persistent supply to the aneurysm despite coverage with PED (black arrow).
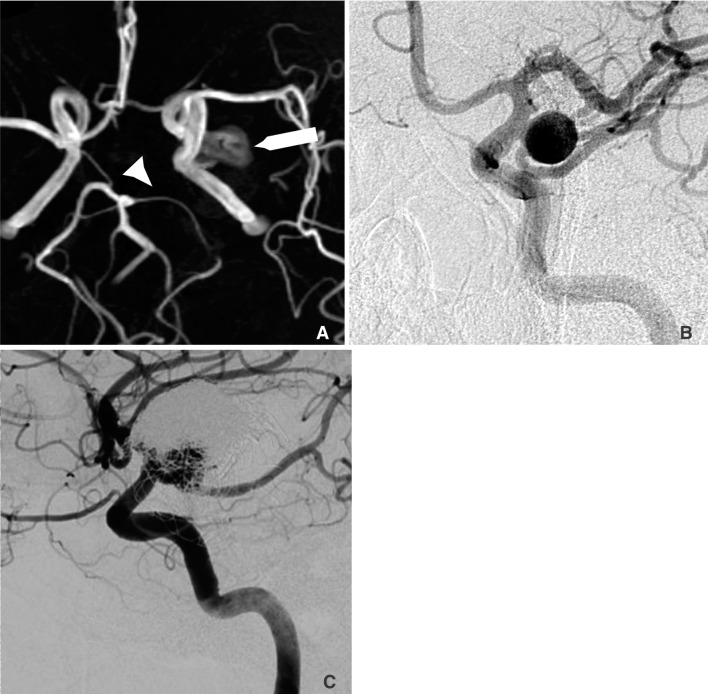
Fig. 3 Patient 3. (A) Pre-treatment magnetic resonance angiography showing the left-sided aneurysm (long arrow), and the atrophic right P1 segment (arrow head) associated with fetal-type circulation; (B) pre-treatment digital subtraction angiography showing that the aneurysm received supply from both the internal carotid artery and the fetal posterior communicating artery; (C) digital subtraction angiography performed six months after the placement of one pipeline device showing persistent contrast filling of the slightly enlarged aneurysm with evidence of coil compaction.
Cited by 1 articles
-
A Case of Ruptured Blood Blister-like Aneurysm Treated with Pipeline Embolization Device: Clinical Significance of Fetal-type Posterior Communicating Artery
Ki-Su Park, Dong-Hun Kang, Won-Soo Son, Jaechan Park, Young-Sun Kim, Byung Moon Kim
Neurointervention. 2017;12(1):40-44. doi: 10.5469/neuroint.2017.12.1.40.
Reference
-
1. Fiorella D, Kelly ME, Albuquerque FC, Nelson PK. Curative reconstruction of a giant midbasilar trunk aneurysm with the pipeline embolization device. Neurosurgery. 2009; 64:212–217. PMID: 19057425.
Article2. Fiorella D, Woo HH, Albuquerque FC, Nelson PK. Definitive reconstruction of circumferential, fusiform intracranial aneurysms with the pipeline embolization device. Neurosurgery. 2008; 62:1115–1120. PMID: 18580809.
Article3. Lylyk P, Miranda C, Ceratto R, Ferrario A, Scrivano E, Luna HR, et al. Curative endovascular reconstruction of cerebral aneurysms with the pipeline embolization device: the Buenos Aires experience. Neurosurgery. 2009; 64:632–642. PMID: 19349825.4. Leung GK, Tsang AC, Lui WM. Pipeline embolization device for intracranial aneurysm: a systematic review. Clin Neuroradiol. 2012; 22:295–303. PMID: 23124329.
Article5. Yu SC, Kwok CK, Cheng PW, Chan KY, Lau SS, Lui WM, et al. Intracranial aneurysms: midterm outcome of pipeline embolization device--a prospective study in 143 patients with 178 aneurysms. Radiology. 2012; 265:893–901. PMID: 22996749.
Article6. Ryu CW, Kwon OK, Koh JS, Kim EJ. Analysis of aneurysm rupture in relation to the geometric indices: aspect ratio, volume, and volume-to-neck ratio. Neuroradiology. 2011; 53:883–889. PMID: 21107548.
Article7. McAuliffe W, Wycoco V, Rice H, Phatouros C, Singh TJ, Wenderoth J. Immediate and midterm results following treatment of unruptured intracranial aneurysms with the pipeline embolization device. AJNR Am J Neuroradiol. 2012; 33:164–670. PMID: 21979492.
Article8. Nelson PK, Lylyk P, Szikora I, Wetzel SG, Wanke I, Fiorella D. The pipeline embolization device for the intracranial treatment of aneurysms trial. AJNR Am J Neuroradiol. 2011; 32:34–40. PMID: 21148256.
Article9. O'Kelly CJ, Spears J, Chow M, Wong J, Boulton M, Weill A, et al. Canadian Experience with the Pipeline Embolization Device for Repair of Unruptured Intracranial Aneurysms. AJNR Am J Neuroradiol. 2013; 34:381–387. PMID: 22859284.10. Golshani K, Ferrell A, Zomorodi A, Smith TP, Britz GW. A review of the management of posterior communicating artery aneurysms in the modern era. Surg Neurol Int. 2010; 1:88. PMID: 21206898.
Article11. Campi A, Ramzi N, Molyneux AJ, Summers PE, Kerr RS, Sneade E, et al. Retreatment of ruptured cerebral aneurysms in patients randomized by coiling or clipping in the International Subarachnoid Aneurysm Trial (ISAT). Stroke. 2007; 38:1538–1544. PMID: 17395870.
Article12. Songsaeng D, Geibprasert S, ter Brugge KG, Willinsky R, Tymianski M, Krings T. Impact of individual intracranial arterial aneurysm morphology on initial obliteration and recurrence rates of endovascular treatments: a multivariate analysis. J Neurosurg. 2011; 114:994–1002. PMID: 20932093.
Article13. Zada G, Breault J, Liu CY, Khalessi AA, Larsen DW, Teitelbaum GP, et al. Internal carotid artery aneurysms occurring at the origin of fetal variant posterior cerebral arteries. Neurosurgery. 2008; 63:ONS55–ONS62. PMID: 18728604.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Salvage flow diverter stent across the posterior communicating artery for persistent retrograde filling of a giant internal carotid artery aneurysm after parent vessel occlusion
- Double-Balloon-Assisted Coiling for Wide-Necked Posterior Communicating Artery Aneurysms with a Fetal-Type Variant of the Posterior Cerebral Artery: A Case Series
- Clinical Analysis of the Pattern of Anterior-Posterior Circulation in Patients with Posterior Communicating Artery Aneurysm
- True Posterior Communicating Artery Aneurysm
- Multiple Intracranial Aneurysms: A Case Report of Patient with Nine Multiple Intracranial Aneurysms
