Clinical features of thoracic endometriosis: A single center analysis
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. beanpearl@yuhs.ac
- KMID: 2148935
- DOI: http://doi.org/10.5468/ogs.2015.58.3.223
Abstract
OBJECTIVE
To analyze the diagnostic profiles and treatment outcomes of patients with thoracic endometriosis at a university hospital.
METHODS
A retrospective review of medical records was performed for patients diagnosed with thoracic endometriosis at Gangnam Severance Hospital, Yonsei University College of Medicine, between January 2007 and January 2014.
RESULTS
Fifteen patients (median age, 35 years; range, 23-48 years) were evaluated. Patients presented with catamenial hemoptysis (n=8), or catamenial pneumothorax (n=7). Patients with catamenial pneumothorax were significantly older than those presenting with hemoptysis (P=0.0002). Only 3 patients (20%) had coexisting pelvic endometriosis. All patients underwent chest computed tomography; lesions were shown to predominantly affect the right lung (right lung, n=13, 86.7%; left lung, n=2, 13.3%), and were mainly distributed on the right upper lobe (n=9, 60%). Ten patients underwent video-assisted thoracoscopic surgery, and 1 patient underwent a thoracotomy. Intraoperatively, endometriosis-specific findings were observed in 8/11 patients (72.7%); a further 5/11 patients (45.4%) had histologically detectable endometriosis. Over the follow-up period (mean, 18.4 months; range, 2-65 months) 5/15 patients (33%) had clinical signs of recurrence. Recurrence was not detected in any of the 5 catamenial pneumothorax patients that received adjuvant hormonal therapy after surgery.
CONCLUSION
The diagnosis and management of thoracic endometriosis requires a multidisciplinary approach, based upon skillful differential diagnosis, and involving careful gynecologic evaluation and assessment of the cyclicity of pulmonary symptoms. Imaging findings are non-specific, though there may be laterality towards the right lung. Since symptom recurrence is more common in those with presenting with pneumothorax, post-operative adjuvant medical therapy is recommended.
MeSH Terms
Figure
-

Fig. 1 Intraoperative photos from a patient presenting with catamenial hemoptysis (P4). (A) Multiple endometriotic spots and a hemorrhagic appearance, observed on the surface of the left upper lobe. (B) After lobectomy, the left upper lobe (dimensions, 18×12×2.5 cm; weight, 160 g) shows significant hemorrhagic areas. Intraoperative photos from a patient presenting with catamenial pneumothorax (P13). (C) Multiple 1 to 5 mm diaphragmatic holes are found on the central tendon of the diaphragm, with multiple endometriotic spots. (D) The specimen after diaphragmatic resection (dimensions, 5×3×0.3 cm). Histology of the resected diaphragm showed the multiple nodules and endometrial stromal cells.
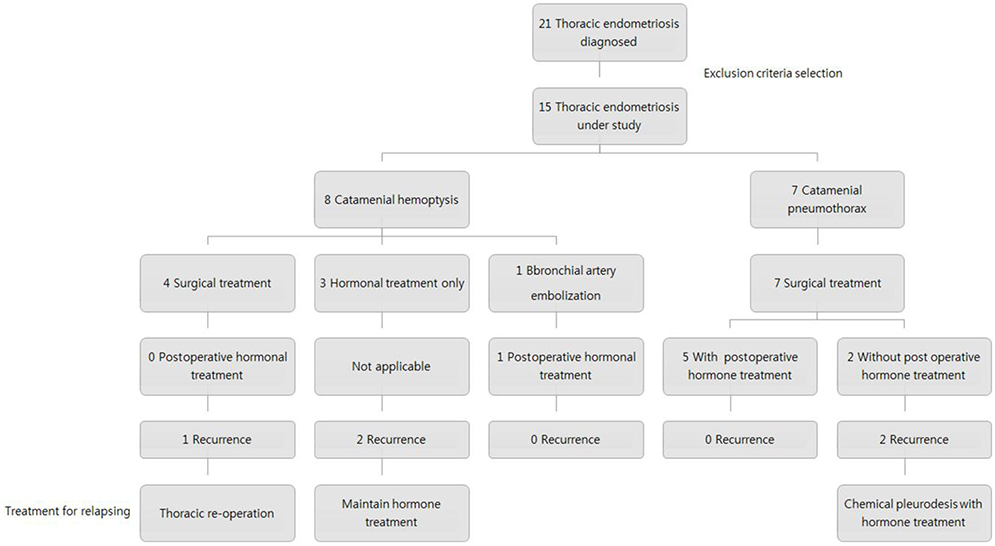
Fig. 2 Algorithm summarizing thoracic endometriosis management protocols employed at our institute. BAE, bronchial artery embolization.
Cited by 1 articles
-
Recurrent hemoptysis in a 26-year-old woman with a ground-glass opacity lesion of the lung
Jong Ha Kim, Sin-Youl Park
Yeungnam Univ J Med. 2019;37(1):59-62. doi: 10.12701/yujm.2019.00304.
Reference
-
1. Attaran M, Falcone T, Goldberg J. Endometriosis: still tough to diagnose and treat. Cleve Clin J Med. 2002; 69:647–653.2. Szamatowicz M. Endometriosis: still an enigmatic disease. What are the causes, how to diagnose it and how to treat successfully? Gynecol Endocrinol. 2008; 24:535–536.3. Augoulea A, Lambrinoudaki I, Christodoulakos G. Thoracic endometriosis syndrome. Respiration. 2008; 75:113–119.4. Hilaris GE, Payne CK, Osias J, Cannon W, Nezhat CR. Synchronous rectovaginal, urinary bladder, and pulmonary endometriosis. JSLS. 2005; 9:78–82.5. Visouli AN, Darwiche K, Mpakas A, Zarogoulidis P, Papagiannis A, Tsakiridis K, et al. Catamenial pneumothorax: a rare entity? Report of 5 cases and review of the literature. J Thorac Dis. 2012; 4:Suppl 1. 17–31.6. Simoglou C, Zarogoulidis P, Machairiotis N, Porpodis K, Simoglou L, Mitrakas A, et al. Abdominal wall endometrioma mimicking an incarcerated hernia: a case report. Int J Gen Med. 2012; 5:569–571.7. Veeraswamy A, Lewis M, Mann A, Kotikela S, Hajhosseini B, Nezhat C. Extragenital endometriosis. Clin Obstet Gynecol. 2010; 53:449–466.8. Bagan P, Berna P, Assouad J, Hupertan V, Le Pimpec Barthes F, Riquet M. Value of cancer antigen 125 for diagnosis of pleural endometriosis in females with recurrent pneumothorax. Eur Respir J. 2008; 31:140–142.9. Haga T, Kataoka H, Ebana H, Otsuji M, Seyama K, Tatsumi K, et al. Thoracic endometriosis-related pneumothorax distinguished from primary spontaneous pneumothorax in females. Lung. 2014; 192:583–587.10. Okeke TC, Ikeako LC, Ezenyeaku CC. Endometriosis. Niger J Med. 2011; 20:191–199.11. Huang H, Li C, Zarogoulidis P, Darwiche K, Machairiotis N, Yang L, et al. Endometriosis of the lung: report of a case and literature review. Eur J Med Res. 2013; 18:13.12. Channabasavaiah AD, Joseph JV. Thoracic endometriosis: revisiting the association between clinical presentation and thoracic pathology based on thoracoscopic findings in 110 patients. Medicine. 2010; 89:183–188.13. Yoshioka H, Fukui T, Mori S, Usami N, Nagasaka T, Yokoi K. Catamenial pneumothorax in a pregnant patient. Jpn J Thorac Cardiovasc Surg. 2005; 53:280–282.14. Orriols R, Munoz X, Alvarez A, Sampol G. Chest CT scanning: utility in lung endometriosis. Respir Med. 1998; 92:876–877.15. Suginami H. A reappraisal of the coelomic metaplasia theory by reviewing endometriosis occurring in unusual sites and instances. Am J Obstet Gynecol. 1991; 165:214–218.16. Rousset-Jablonski C, Alifano M, Plu-Bureau G, Camilleri-Broet S, Rousset P, Regnard JF, et al. Catamenial pneumothorax and endometriosis-related pneumothorax: clinical features and risk factors. Hum Reprod. 2011; 26:2322–2329.17. Tripp HF, Obney JA. Consideration of anatomic defects in the etiology of catamenial pneumothorax. J Thorac Cardiovasc Surg. 1999; 117:632–633.18. Joseph J, Sahn SA. Thoracic endometriosis syndrome: new observations from an analysis of 110 cases. Am J Med. 1996; 100:164–170.19. Shin SP, Park CY, Song JH, Kim HM, Min D, Lee SH, et al. A case of catamenial hemoptysis treated by bronchial artery embolization. Tuberc Respir Dis. 2014; 76:233–236.20. Lee DY, Bae DS, Yoon BK, Choi D. Post-operative cyclic oral contraceptive use after gonadotrophin-releasing hormone agonist treatment effectively prevents endometrioma recurrence. Hum Reprod. 2010; 25:3050–3054.
