Ann Surg Treat Res.
2015 Dec;89(6):334-337. 10.4174/astr.2015.89.6.334.
Neonatal vitelline vein aneurysm with thrombosis: prompt treatment should be needed
- Affiliations
-
- 1Department of Pediatric Surgery, Pusan National University Yangsan Hospital, Yangsan, Korea.
- 2Department of Pediatric Surgery, Seoul National University Children's Hospital, Seoul, Korea. spkhy02@snu.ac.kr
- 3Department of Pediatrics, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- KMID: 2148310
- DOI: http://doi.org/10.4174/astr.2015.89.6.334
Abstract
- Vitelline veins are a pair of embryonic structures. The veins develop the portal vein system. Serious problems occur if the vitelline vein does not regress and becomes an aneurysm. Thrombus formation in the vitelline vein aneurysm could lead to portal vein thrombosis and portal hypertension unless promptly and correctly treated. Though vitelline vein aneurysm is an extremely rare anomaly, it rapidly progresses to portal vein thrombosis that requires prompt diagnosis and treatment. We reported a case of neonatal vitelline vein aneurysm and thrombosis that was cured by prompt operation.
MeSH Terms
Figure
-
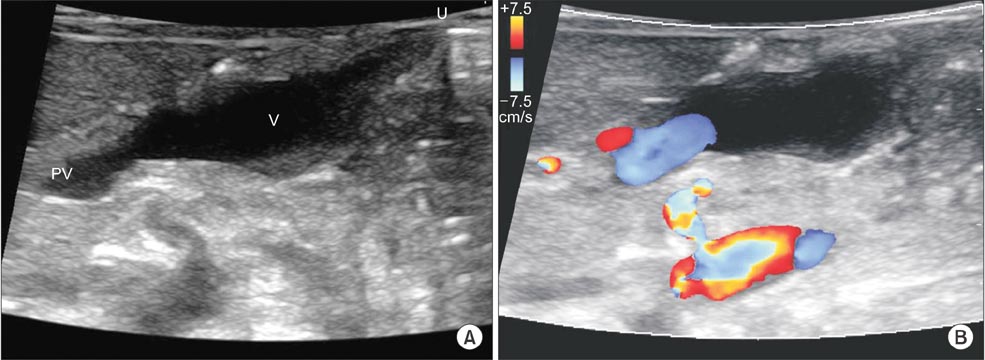
Fig. 1 Ultrasonographic findings on the day of birth: (A) an elongated aneurismal tubular structure (V: vitelline vein aneurysm) with connection to the main portal vein (PV) coursing towards the umbilicus (U), (B) Color Doppler ultrasonography showed patent portal vein flow.

Fig. 2 Three-dimensional CT abdominal findings: abnormal tubular dilatated vascular structure and intraluminal thrombus, vitelline vein aneurysm (black arrowheads), connected with superior mesenteric vein (white arrow), splenic vein (black arrow) and portal vein (white arrowheads).
Reference
-
1. Kang KW, Sung DJ, Park BJ, Kim MJ, Cho SB. Aneurysmal dilatation of persistent vitelline vein with thrombus in a neonate. Pediatr Radiol. 2014; 44:893–896.2. Kivilevitch Z, Achiron R. Fetal extrahepatic vitelline vein aneurysm mimicking an umbilical vein varix. J Ultrasound Med. 2010; 29:1651–1656.3. Scalabre A, Gorincour G, Hery G, Gamerre M, Guys JM, de Lagausie P. Evolution of congenital malformations of the umbilical-portal-hepatic venous system. J Pediatr Surg. 2012; 47:1490–1495.4. Benoist G, Gauthier F, Belloy F, Laloum D, Herlicoviez M, Dreyfus M. Antenatal sonographic features of aneurysmal dilatation of a vitelline vein. Ultrasound Obstet Gynecol. 2007; 29:708–711.5. Lee SW, Kim MY, Kim JE, Chung JH, Lee HJ, Yoon JY. Clinical characteristics and outcomes of antenatal fetal intra-abdominal umbilical vein varix detection. Obstet Gynecol Sci. 2014; 57:181–186.6. Moon SB, Park KW, Jung SE. Abnormal direct entry of the umbilical vein into the portal vein: report of a case. Pediatr Surg Int. 2008; 24:1243–1245.7. Hery G, Quarello E, Gorincour G, Franchi S, Gauthier F, de Lagausie P. Extrahepatic vitelline vein aneurysm: prenatal diagnosis and follow up. J Pediatr Surg. 2013; 48:e1–e4.8. Beraud E, Rozel C, Milon J, Darnault P. Umbilical vein varix: importance of anteand post-natal monitoring by ultrasound. Diagn Interv Imaging. 2015; 96:21–26.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiologic Findings of Neonatal Cerebral Infarction related with Portal Vein Thrombosis: Case Report
- Venous Aneurysm of the Right External Jugular Vein
- Treatment of Subclavian Vein Thrombosis: Medial Claviculectomy and Internal Jugular Vein Transposition
- Popliteal Artery Aneurysm Presenting as Acute Deep Vein Thrombosis
- Unusual Presentation of a Cervical Mass Revealed as External Jugular Venous Aneurysm
