Ann Rehabil Med.
2015 Oct;39(5):793-799. 10.5535/arm.2015.39.5.793.
Effect of Repetitive Transcranial Magnetic Stimulation on Patients With Dysarthria After Subacute Stroke
- Affiliations
-
- 1Department of Rehabilitation Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. mhchun@amc.seoul.kr
- 2Rehabilitation Center, Union Hospital, Daegu, Korea.
- KMID: 2148211
- DOI: http://doi.org/10.5535/arm.2015.39.5.793
Abstract
OBJECTIVE
To evaluate whether repetitive transcranial magnetic stimulation (rTMS) could improve dysarthria in stroke patients at the subacute stage.
METHODS
This study was a prospective, randomized, double-blind controlled trial. Patients who had unilateral middle cerebral artery infarction were enrolled. In patients in the rTMS group, we found hot spots by searching for the evoked motor potential of the orbicularis oris on the non-affected side. We performed rTMS at a low frequency (1 Hz), 1,500 stimulations/day, 5 days a week for 2 weeks on the hotspots. We used the same protocol in the sham stimulation group patients as that in the rTMS group, except that the angle of the coil was perpendicular to the skull rather than tangential to it. The patients in both groups received speech therapy for 30 minutes, 5 days a week from a skilled speech therapist. The speech therapist measured the Urimal Test of Articulation and Phonology, alternative motion rates, sequential motion rates, and maximal phonation time before and after intervention sessions.
RESULTS
Forty-two patients were enrolled in this study and 20 completed the study. Statistical analysis revealed significant improvements on the dysarthria scales in both groups. The sequential motion rate (SMR)-PTK showed significantly greater improvement in the rTMS group patients than in the sham stimulation group.
CONCLUSION
Patients in the rTMS group showed greater improvement in articulation than did patients in the sham rTMS group. Therefore, rTMS can have a synergistic effect with speech therapy in treating dysarthria after stroke.
MeSH Terms
Figure
-
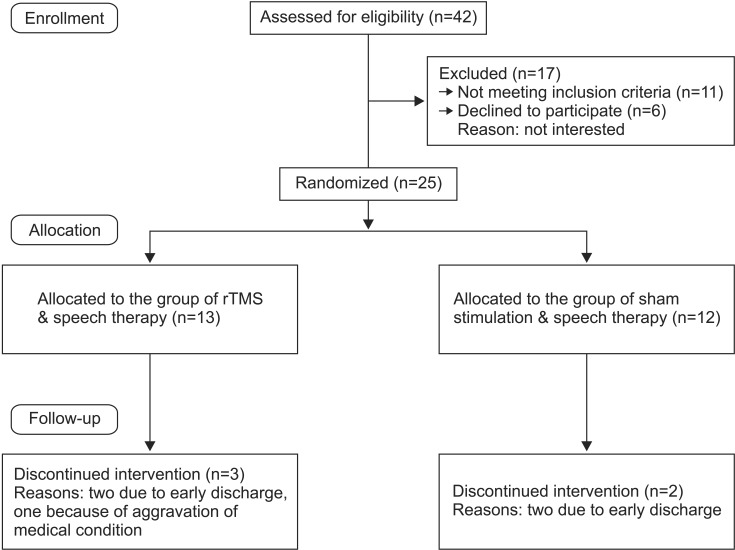
Fig. 1 Flowchart of patient recruitment.
Cited by 1 articles
-
Correlation Between Articulatory Diadochokinetic Parameters and Dysphagia Parameters in Subacute Stroke Patients
Back Min Oh, Hyun Seok, Sang-Hyun Kim, Seung Yeol Lee, Su Jung Park, Beom Jin Kim, Hyun Jung Kim
Ann Rehabil Med. 2023;47(3):192-204. doi: 10.5535/arm.23018.
Reference
-
1. Yorkston KM, Beukelman DR. Ataxic dysarthria: treatment sequences based on intelligibility and prosodic considerations. J Speech Hear Disord. 1981; 46:398–404. PMID: 7300267.2. Martin BJ, Corlew MM. The incidence of communication disorders in dysphagic patients. J Speech Hear Disord. 1990; 55:28–32. PMID: 2299837.
Article3. Flowers HL, Silver FL, Fang J, Rochon E, Martino R. The incidence, co-occurrence, and predictors of dysphagia, dysarthria, and aphasia after first-ever acute ischemic stroke. J Commun Disord. 2013; 46:238–248. PMID: 23642855.
Article4. Brady MC, Clark AM, Dickson S, Paton G, Barbour RS. The impact of stroke-related dysarthria on social participation and implications for rehabilitation. Disabil Rehabil. 2011; 33:178–186. PMID: 20831375.
Article5. Sellars C, Hughes T, Langhorne P. Speech and language therapy for dysarthria due to non-progressive brain damage (review). Chichester:: John Wiley & Sons;2009.6. Alonso-Alonso M, Fregni F, Pascual-Leone A. Brain stimulation in poststroke rehabilitation. Cerebrovasc Dis. 2007; 24(Suppl 1):157–166. PMID: 17971652.
Article7. Lefaucheur JP. Stroke recovery can be enhanced by using repetitive transcranial magnetic stimulation (rTMS). Neurophysiol Clin. 2006; 36:105–115. PMID: 17046605.8. Pascual-Leone A, Amedi A, Fregni F, Merabet LB. The plastic human brain cortex. Annu Rev Neurosci. 2005; 28:377–401. PMID: 16022601.
Article9. Peinemann A, Reimer B, Loer C, Quartarone A, Munchau A, Conrad B, et al. Long-lasting increase in corticospinal excitability after 1800 pulses of subthreshold 5 Hz repetitive TMS to the primary motor cortex. Clin Neurophysiol. 2004; 115:1519–1526. PMID: 15203053.
Article10. Maeda F, Keenan JP, Tormos JM, Topka H, Pascual-Leone A. Modulation of corticospinal excitability by repetitive transcranial magnetic stimulation. Clin Neurophysiol. 2000; 111:800–805. PMID: 10802449.
Article11. Muellbacher W, Ziemann U, Boroojerdi B, Hallett M. Effects of low-frequency transcranial magnetic stimulation on motor excitability and basic motor behavior. Clin Neurophysiol. 2000; 111:1002–1007. PMID: 10825706.
Article12. Hsu WY, Cheng CH, Liao KK, Lee IH, Lin YY. Effects of repetitive transcranial magnetic stimulation on motor functions in patients with stroke: a meta-analysis. Stroke. 2012; 43:1849–1857. PMID: 22713491.13. You DS, Chun MH, Kim DY, Han EY, Jung SE. The effects of transcranial direct current stimulation on dysarthria in stroke patients. J Korean Acad Rehabil Med. 2010; 34:10–14.14. Takeuchi N, Chuma T, Matsuo Y, Watanabe I, Ikoma K. Repetitive transcranial magnetic stimulation of contralesional primary motor cortex improves hand function after stroke. Stroke. 2005; 36:2681–2686. PMID: 16254224.
Article15. Kim YH, You SH, Ko MH, Park JW, Lee KH, Jang SH, et al. Repetitive transcranial magnetic stimulationinduced corticomotor excitability and associated motor skill acquisition in chronic stroke. Stroke. 2006; 37:1471–1476. PMID: 16675743.
Article16. Khedr EM, Etraby AE, Hemeda M, Nasef AM, Razek AA. Long-term effect of repetitive transcranial magnetic stimulation on motor function recovery after acute ischemic stroke. Acta Neurol Scand. 2010; 121:30–37. PMID: 19678808.
Article17. Talelli P, Greenwood RJ, Rothwell JC. Exploring Theta Burst Stimulation as an intervention to improve motor recovery in chronic stroke. Clin Neurophysiol. 2007; 118:333–342. PMID: 17166765.
Article18. Fimbel EJ, Domingo PP, Lamoureux D, Beuter A. Automatic detection of movement disorders using recordings of rapid alternating movements. J Neurosci Methods. 2005; 146:183–190. PMID: 16054508.
Article19. Kent RD, Weismer G, Kent JF, Vorperian HK, Duffy JR. Acoustic studies of dysarthric speech: methods, progress, and potential. J Commun Disord. 1999; 32:141–180. 183–186. PMID: 10382143.20. Tjaden K, Watling E. Characteristics of diadochokinesis in multiple sclerosis and Parkinson's disease. Folia Phoniatr Logop. 2003; 55:241–259. PMID: 12931058.
Article21. Urban PP, Rolke R, Wicht S, Keilmann A, Stoeter P, Hopf HC, et al. Left-hemispheric dominance for articulation: a prospective study on acute ischaemic dysarthria at different localizations. Brain. 2006; 129(Pt 3):767–777. PMID: 16418180.
Article22. Seikel JA, King DW, Drumright DG. Anatomy & physiology for speech, language, and hearing. 2nd ed. San Diego: Singular Publishing;2000.23. Borden GJ, Harris KS, Raphael LJ. Speech science primer: physiology, acoustics, and perception of speech. 3rd ed. Baltimore: Lippincott Williams & Wilkins;1994.24. Liegeois FJ, Morgan AT. Neural bases of childhood speech disorders: lateralization and plasticity for speech functions during development. Neurosci Biobehav Rev. 2012; 36:439–458. PMID: 21827785.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Application of Non-invasive Brain Stimulation on Dysphagia after Stroke
- Effect of Low-Frequency rTMS and NMES on Subacute Unilateral Hemispheric Stroke With Dysphagia
- Comparison of Effects of Repetitive Transcranial Magnetic Stimulation with High- or Low-frequency on Visuospatial Neglect in Stroke Patients
- Effect of Repetitive Transcranial Magnetic Stimulation According to the Stimulation Site in Stroke Patients With Dysphagia
- Stroke Update 2011: Stroke Rehabilitation
