Huge Multilobulated Left Ventricular Outflow Tract Pseudoaneurysm Presenting with Ventricular Tachycardia
- Affiliations
-
- 1Department of Cardiology, U N Mehta Institute of Cardiology and Research Centre, Ahmedabad, Gujarat, India. dr.rajivkharwar@gmail.com
- KMID: 2144462
- DOI: http://doi.org/10.4250/jcu.2015.23.4.276
Abstract
- No abstract available.
MeSH Terms
Figure
-

Fig. 1 The presenting electrocardiogram of the patient showing monomorphic ventricular tachycardia originating from the left ventricular outflow tract region (A). Post direct current cardioversion, patient regained normal sinus rhythm but with bifascicular block in the form of right bundle branch block with left anterior hemiblock (B). aVR: augmented vector right, aVL: augmented vector left, aVF: augmented vector foot.
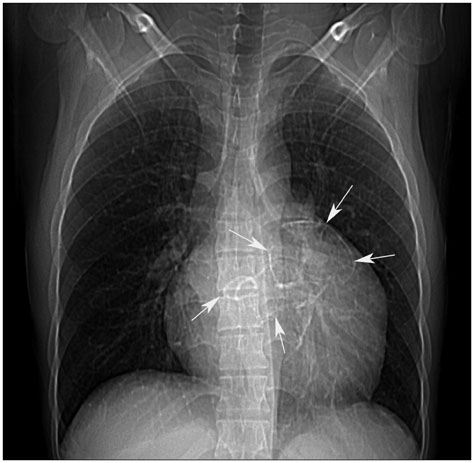
Fig. 2 Chest X-ray showing cardiomegaly with a bulge at the upper left cardiac border along with multiple calcified round to oval shadows (white arrows) within the cardiac silhouette.
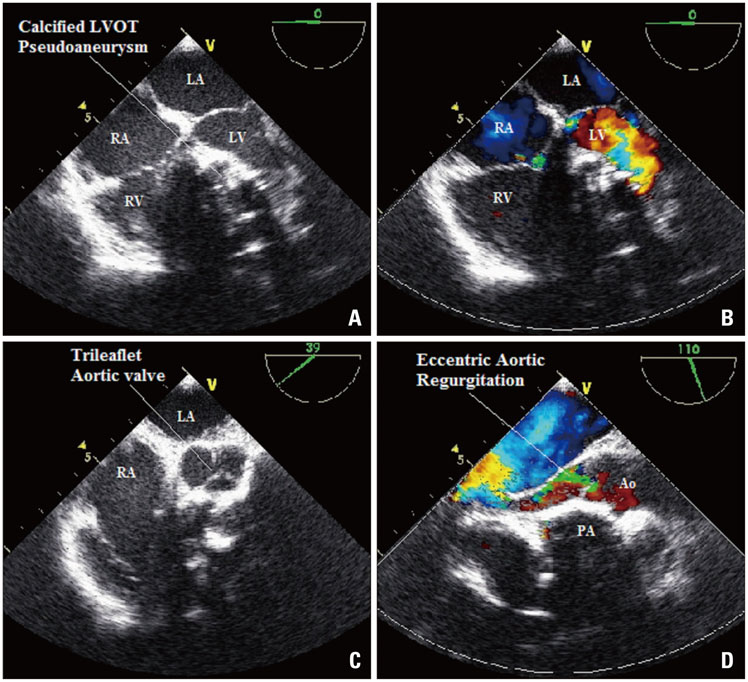
Fig. 3 Transesophageal echocardiography with color Doppler. The mid esophageal four chamber view showing a large calcified mass in the basal septal region compressing the LV cavity (A) leading to mild mitral regurgitation (B). The aortic valve was tri-leaflet as seen in the basal short axis view (C) and there was moderate aortic valve regurgitation in the LV out flow view (D). Ao: aorta, LA: left atrium, LV: left ventricle, LVOT: left ventricular outflow tract, PA: pseudoaneurysm, RA: right atrium, RV: right ventricle.
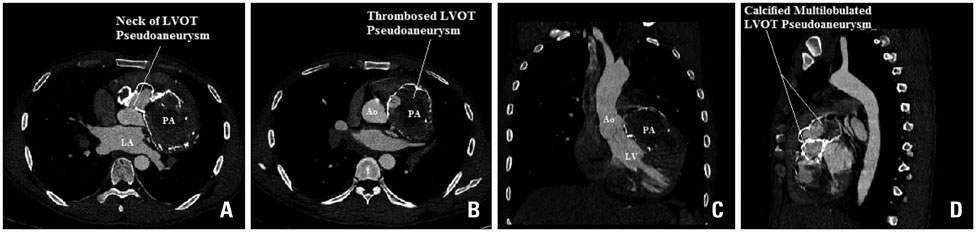
Fig. 4 Multidetector computed tomography. The communication of the pseudoaneurysm with the LVOT can be clearly seen in the axial section (A). The multilobulated nature, the calcified rims and the thrombosed lumen of the pseudoaneurysm can also be seen in the axial section (B), coronal section (C) and the sagittal section (D). Ao: aorta, LA: left atrium, LV: left ventricle, LVOT: left ventricular outflow tract, PA: pseudoaneurysm.

Fig. 5 Invasive left ventriculography in the right anterior oblique projection (A) and in the left anterior oblique (LAO) projection with cranial angulation (B) showing the calcified, multilobulated LVOT pseudoaneurysm filling partially due to the thrombosed internal lumen. Invasive coronary angiogram in the straight anteroposterior projection (C) and in the LAO projection with caudal angulation (D) showing the extrinsic compression of the proximal LAD coronary artery by the pseudoaneurysm. Ao: aorta, LAD: left anterior descending, LV: left ventricle, LVOT: left ventricular outflow tract.
Reference
-
1. Afridi I, Apostolidou MA, Saad RM, Zoghbi WA. Pseudoaneurysms of the mitral-aortic intervalvular fibrosa: dynamic characterization using transesophageal echocardiographic and Doppler techniques. J Am Coll Cardiol. 1995; 25:137–145.2. Jha AK, Pandey R, Gharde P, Devagourou V, Kiran U. Idiopathic left ventricular outflow tract pseudoaneurysm. Ann Card Anaesth. 2013; 16:209–211.3. Kaul S, Josephson MA, Tei C, Wittig JH, Millman J, Shah PM. Atypical echocardiographic and angiographic presentation of a postoperative pseudoaneurysm of the left ventricle after repair of a true aneurysm. J Am Coll Cardiol. 1983; 2:780–784.4. Yeo TC, Malouf JF, Reeder GS, Oh JK. Clinical characteristics and outcome in postinfarction pseudoaneurysm. Am J Cardiol. 1999; 84:592–595.5. Da Col U, Ramoni E, Di Bella I, Ragni T. An unusual left ventricular outflow pseudoaneurysm: usefulness of echocardiography and multidetector computed tomography for surgical repair. Cardiovasc Intervent Radiol. 2009; 32:188–191.6. Savage MP, Hopkins JT, Templeton JY 3rd, Goldburgh WP, Goldberg S. Left ventricular pseudopseudoaneurysm: angiographic features and surgical treatment of impending cardiac rupture. Am Heart J. 1988; 116:864–866.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Idiopathic Polymorphic Ventricular Tachycardia: a “Benign Disease†with a Touch of Bad Luck?
- Giant Cardiac Rhabdomyoma with Mixed Atrial Tachycardia and Nonsustained Ventricular Tachycardia in a Newborn with Tuberous Sclerosis
- Multiple Rhabomyomas in left Ventricular Outflow Tract Combined with Tuberous Sclerosis: A Case Report
- Ventricular Tachycardia in Neonates: A Report of Two Cases and Review of the Literature
- A Rare Case of Unruptured Sinus of Valsalva Aneurysm Obstructing the Right Ventricular Outflow Tract
