J Korean Assoc Oral Maxillofac Surg.
2012 Dec;38(6):354-359. 10.5125/jkaoms.2012.38.6.354.
Investigating the effect of age on skeletal stability after sagittal split ramus osteotomy for mandibular setback
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Kyungpook National University, Daegu, Korea. kwondk@knu.ac.kr
- KMID: 2136972
- DOI: http://doi.org/10.5125/jkaoms.2012.38.6.354
Abstract
OBJECTIVES
The purpose of this study was to investigate whether the age factor would be related with stability of mandibular setback surgery for patients with mandibular prognathism.
MATERIALS AND METHODS
We compared the relapse patterns of 47 patients divided into three age groups (termed younger, adult, and older). The younger group consisted of patients between 15 and 17 years old; the adult group was made up of patients between 21 and 23 years old, and the older group was made up of patients more than 40 years old. The positional change of B point was evaluated at preoperative, postoperative, and follow-up states.
RESULTS
The horizontal relapse ratio was 21.7% in the younger group, 15.3% in the adult group, and 15.7% in the older group. Although relatively higher degrees of relapse were found in the younger group, this increase was not statistically significant. Spearman's correlation analysis was performed to explore other factors contributing to relapse. We subsequently found that the amount of relapse was related to horizontal setback.
CONCLUSION
Although the degree of relapse in younger patients is not significant;y higher compared to other groups. The major contributing factor to relapse after sagittal split ramus osteotomy is amount of setback rather than age when the surgery was performed to patients over than 15 years of age.
Keyword
MeSH Terms
Figure
-

Fig. 1. Lateral cephalograms were obtained before surgery (T0), 2-3 days after surgery (T1), and more than 6 months after surgery (T2).

Fig. 2. Measurement for lateral cephalometric analysis. (N: nasion, S: sella, Po: porion, Or: orbitale, FH: frankfurt)
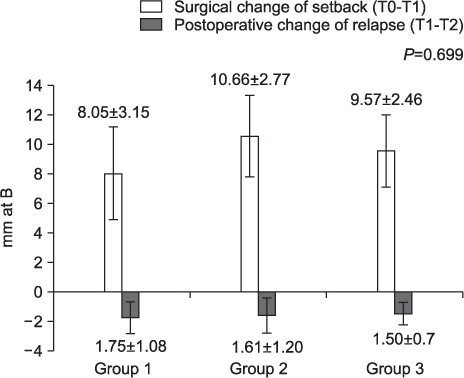
Fig. 3. Comparison of surgical change (B [x]) and relapse according to the groups.
Reference
-
1. Proffit WR, Fields HW Jr, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg. 1998; 13:97–106.2. Lee SJ, Suhr CH. Recognition of malocclusion and orthodontic treatment need of 7~18 year-old korean adolescent. Korean J Orthod. 1994; 24:367–394.3. Yoo YK, Kim NI, Lee HK. A study on the prevalence of malocclusion in 2,378 Yonsei University students. Korean J Orthod. 1971; 2:35–40.4. Choi BH, Min YS, Yi CK, Lee WY. A comparison of the stability of miniplate with bicortical screw fixation after sagittal split setback. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 90:416–419.
Article5. Harada K, Enomoto S. Stability after surgical correction of mandibular prognathism using the sagittal split ramus osteotomy and fixation with poly-L-lactic acid (PLLA) screws. J Oral Maxillofac Surg. 1997; 55:464–468.
Article6. Ayoub AF, Millett DT, Hasan S. Evaluation of skeletal stability following surgical correction of mandibular prognathism. Br J Oral Maxillofac Surg. 2000; 38:305–311.
Article7. Kim CH, Lee JH, Cho JY, Lee JH, Kim KW. Skeletal stability after simultaneous mandibular angle resection and sagittal split ramus osteotomy for correction of mandible prognathism. J Oral Maxillofac Surg. 2007; 65:192–197.
Article8. Kim MJ, Kim SG, Park YW. Positional stability following intentional posterior ostectomy of the distal segment in bilateral sagittal split ramus osteotomy for correction of mandibular prognathism. J Craniomaxillofac Surg. 2002; 30:35–40.
Article9. Choi BH, Zhu SJ, Han SG, Huh JY, Kim BY, Jung JH. The need for intermaxillary fixation in sagittal split osteotomy setbacks with bicortical screw fixation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 100:292–295.
Article10. Joss CU, Thüer UW. Stability of hard tissue profile after mandibular setback in sagittal split osteotomies: a longitudinal and long-term follow-up study. Eur J Orthod. 2008; 30:352–358.
Article11. Mobarak KA, Krogstad O, Espeland L, Lyberg T. Long-term stability of mandibular setback surgery: a follow-up of 80 bilateral sagittal split osteotomy patients. Int J Adult Orthodon Orthognath Surg. 2000; 15:83–95.12. Schatz JP, Tsimas P. Cephalometric evaluation of surgical-orthodontic treatment of skeletal Class III malocclusion. Int J Adult Orthodon Orthognath Surg. 1995; 10:173–180.13. Wolford LM, Schendel SA, Epker BN. Surgical-orthodontic correction of mandibular deficiency in growing children (long term treatment results). J Maxillofac Surg. 1979; 7:61–72.14. Huang CS, Ross RB. Surgical advancement of the retrognathic mandible in growing children. Am J Orthod. 1982; 82:89–103.
Article15. Schendel SA, Wolford LM, Epker BN. Mandibular deficiency syndrome. III. Surgical advancement of the deficient mandible in growing children: treatment results in twelve patients. Oral Surg Oral Med Oral Pathol. 1978; 45:364–377.
Article16. Lewis AB, Roche AF. Late growth changes in the craniofacial skeleton. Angle Orthod. 1988; 58:127–135.17. Miloro M, Ghali GE, Larsen PE, Waite P. In: Peterson's principles of oral and maxillofacial surgery. 2nd ed. Hamilton, London: BC Decker; 2004. pp. 6-7.18. Trauner R, Obwegeser H. Zur operations technik bei der progenie und anderen unterkieferanomalien. Dtsch Zahn Mund-und Kieferheilk. 1955; 23:1–26.19. Trauner R, Obwegeser H. The surgical correction of mandibular prognathism and retrognathisa with consideration of genioplasty. I. Surgical procedures to correct mandibular prognathism and reshaping of the chin. Oral Surg Oral Med Oral Pathol. 1957; 10:677–689.20. Spiessl B. In: Osteosynthese bei sagittaler osteotomie nach Obwegeser/Dal Pont. Stuttgart: Fortschritte der Kiefer-und Gesichtschirurgie; 1974.21. Ochs MW. Bicortical screw stabilization of sagittal split osteotomies. J Oral Maxillofac Surg. 2003; 61:1477–1484.
Article22. Stroster TG, Pangrazio-Kulbersh V. Assessment of condylar position following bilateral sagittal split ramus osteotomy with wire fixation or rigid fixation. Int J Adult Orthodon Orthognath Surg. 1994; 9:55–63.23. Ueki K, Nakagawa K, Marukawa K, Takazakura D, Shimada M, Takatsuka S, et al. Changes in condylar long axis and skeletal stability after bilateral sagittal split ramus osteotomy with poly-L-lactic acid or titanium plate fixation. Int J Oral Maxillofac Surg. 2005; 34:627–634.
Article24. Raveh J, Vuillemin T, Lädrach K, Sutter F. New techniques for reproduction of the condyle relation and reduction of complications after sagittal ramus split osteotomy of the mandible. J Oral Maxillofac Surg. 1988; 46:751–757.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Stability after Surgical Correction of Mandibular Prognathism Using Bilateral Sagittal Split Ramus Osteotomy with Rigid Fixation
- Comparative study of stability and relapse according to fixation method after bilateral sagittal split ramus osteotomies in mandibular prognathic patients
- The study of stability of absorbable internal fixation after mandibular bilateral sagittal split ramal osteotomy
- Initial Stability after Bilateral Sagittal Split Ramus Osteotomy Application in Patients with Mandibular Prognathism
- Comparative Study of Skeletal Relapse According to the Fixation Method after BSSRO for Mandibular Setback
