Complete Laryngotracheal Separation Following Attempted Hanging
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Chungnam National University School of Medicine, Daejeon, Korea. yyh9635@cnuh.co.kr
- KMID: 2134603
- DOI: http://doi.org/10.3342/ceo.2012.5.3.177
Abstract
- Laryngotracheal separation (LTS) is the most immediately life-threatening airway injury. LTS is so rare that very few otolaryngologists have experience with it. LTS is one of the diagnostic and therapeutic challenges in airway diseases and its management remains to be established. We experienced a patient with complete LTS after attempted hanging. A high index of suspicion, adequate imaging, prompt airway establishment and early surgical repair are the most vital factors in managing a patient with LTS.
Keyword
MeSH Terms
Figure
-
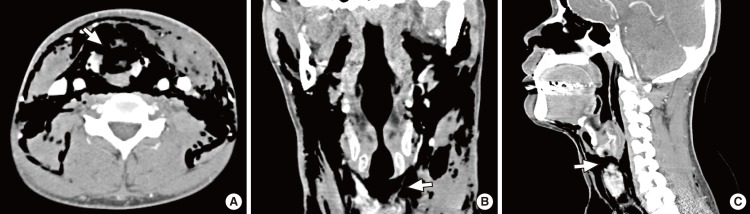
Fig. 1 Preoperative computed tomography (CT) findings. Axial (A), coronal (B), and sagittal (C) image of multi-detector CT reveal extensive subcutaneous emphysema and a complete laryngotracheal separation (arrow) without fractures of the thyroid and cricoid cartilage. Laryngotracheal separation is observed most clearly in the sagittal reconstruction images.
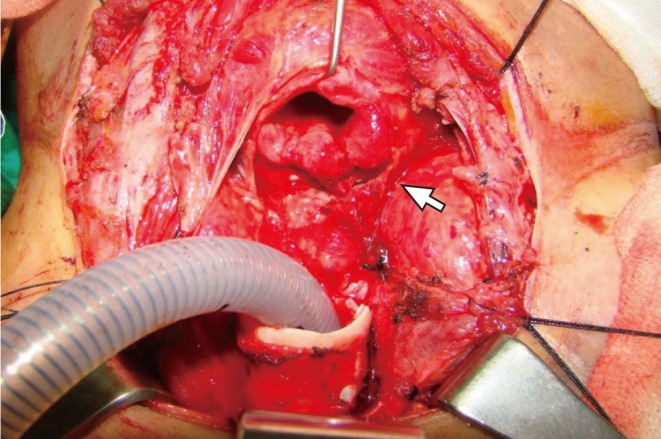
Fig. 2 Intraoperative finding. Complete transection between the cricoid cartilage and the first tracheal ring and stretching of the left recurrent laryngeal nerve (arrow) are observed. Thyroid gland is retracted laterally after dividing the isthmus.

Fig. 3 Postoperative computed tomography (CT) findings. Axial (A), coronal (B), and sagittal (C) image of multi-detector CT taken at postoperative 10 days show complete resolution of subcutaneous emphysema and appropriate reconstruction of laryngotrachea.
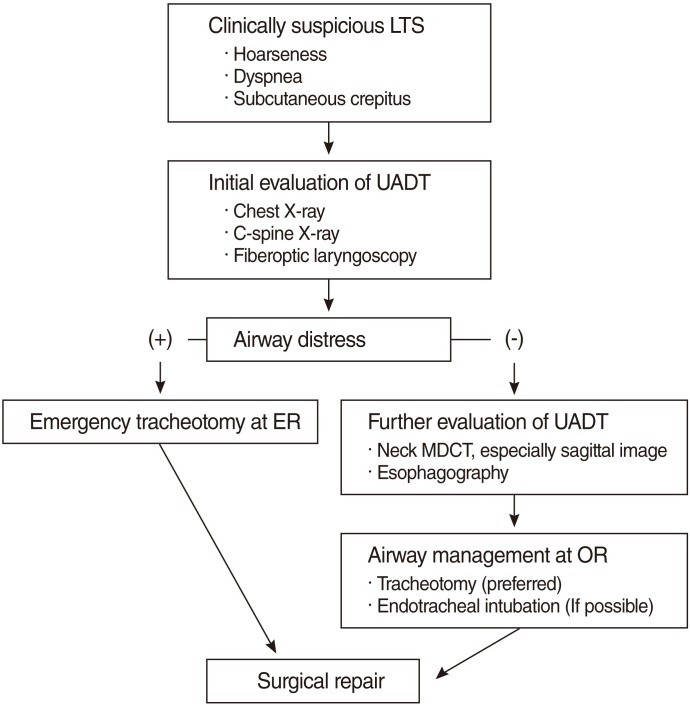
Fig. 4 Proposed algorithm for management of LTS. LTS, laryngotracheal separation; UADT, upper aerodigestive tract; MDCT, multi-detector CT; ER, emergency room; OR, operation room.
Reference
-
1. Singh B, Kumar S, Kumar V. Blunt laryngotracheal injury following accidental strangulation. Injury. 2003; 12. 34(12):937–939. PMID: 14636739.
Article2. McCrystal DJ, Bond C. Cricotracheal separation: a review and a case with bilateral recovery of recurrent laryngeal nerve function. J Laryngol Otol. 2006; 6. 120(6):497–501. PMID: 16606523.
Article3. Aouad R, Moutran H, Rassi S. Laryngotracheal disruption after blunt neck trauma. Am J Emerg Med. 2007; 11. 25(9):1084.e1–1084.e2. PMID: 18022512.
Article4. Costache VS, Renaud C, Brouchet L, Toma T, Le Balle F, Berjaud J, et al. Complete tracheal rupture after a failed suicide attempt. Ann Thorac Surg. 2004; 77(4):1422–1423. PMID: 15063279.
Article5. Borowski DW, Mehrotra P, Tennant D, El Badawey MR, Cameron DS. Unusual presentation of blunt laryngeal injury with cricotracheal disruption by attempted hanging: a case report. Am J Otolaryngol. 2004; May-Jun. 25(3):195–198. PMID: 15124170.
Article6. LeJeune FE Jr. Laryngotracheal separation. Laryngoscope. 1978; 12. 88(12):1956–1962. PMID: 732496.
Article7. Cherry JR, Hammond JE. Transection of the cervical trachea resulting from closed trauma to the neck. J Laryngol Otol. 1984; 1. 98(1):97–100. PMID: 6693810.
Article8. Lupetin AR, Hollander M, Rao VM. CT Evaluation of laryngotracheal trauma. Semin Musculoskelet Radiol. 1998; 2(1):105–116. PMID: 11387094.
Article9. Baumgartner FJ, Ayres B, Theuer C. Danger of false intubation after traumatic tracheal transection. Ann Thorac Surg. 1997; 1. 63(1):227–228. PMID: 8993273.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dysphagia due to Bilateral Recurrent Laryngeal Nerve Injury after Attempted Suicide by Hanging: A Case Report
- Epidemiology of Suicide by Hanging in Fars Province, Iran (2011-2019): A Population-based Cross-sectional Study
- Laryngotracheal Separation for Intractable Aspiration in Severe Brain Damage
- Non-aneurysmal and non-traumatic subarachnoid hemorrhage after attempted suicide by incomplete hanging
- A Case of the Laryngotracheal Separation for Intractable Aspiration in Handicapped Child
