Associated Factors of Nonunion Following Conservative Management of Distal Clavicle Fractures
- Affiliations
-
- 1Department of Orthopedic Surgery, Keimyung University School of Medicine, Daegu, Korea. oscho5362@dsmc.or.kr
- KMID: 2106749
- DOI: http://doi.org/10.4055/jkoa.2015.50.2.137
Abstract
- PURPOSE
The purpose of this study was to evaluate radiological and clinical outcomes and to analyze factors associated with nonunion after conservative management in patients with distal clavicle fracture.
MATERIALS AND METHODS
We analyzed 29 cases. Neer type, coracoclavicular distance (CCD), initial displacement, comminution, union, and presence of bony union were evaluated by plain radiographs. Clinical outcomes according to University of California at Los Angeles (UCLA), American Shoulder and Elbow Surgeons (ASES), and subjective shoulder value (SSV) scores were assessed.
RESULTS
Six cases (20.7%) had developed nonunion. Three cases had asymptomatic nonunion. Mean UCLA, ASES, and SSV scores were 30.9, 88.3, and 87.0 in the union group and 26.7, 76.2, and 70.8 in the nonunion group. Although the nonunion group had inferior clinical outcome compared to the union group, there was no significant difference between the two groups. Older age and more CCD showed correlation with nonunion (p=0.047, p=0.007).
CONCLUSION
Conservative management of distal clavicle fractures provided satisfactory clinical outcomes. The rate of symptomatic nonunion was 10.4%. Occurrence of nonunion showed correlation with older age and more CCD.
MeSH Terms
Figure
-

Figure 1 A 59-year-old man with a right distal clavicle fracture was treated nonoperatively. (A) Initial anteroposterior and oblique radiographs show a Neer type I fracture. (B) Radiographs at 43 months after initial trauma show nonunion. The patient had a normal activity level without pain.

Figure 2 A 62-year-old woman with a left distal clavicle fracture was treated nonoperatively. (A) Initial anteroposterior and oblique radiographs show a Neer type IIB fracture. (B) Radiographs at 7.5 years after initial trauma show nonunion. The patient had a normal activity level without pain.
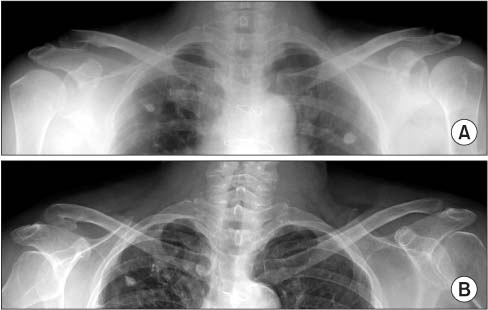
Figure 3 A 73-year-old woman with a right distal clavicle fracture was treated nonoperatively. (A) Initial anteroposterior and oblique radiographs show a Neer type IIB fracture. (B) Radiographs at 7.9 years after initial trauma show union. The patient had a normal activity level without pain.
Cited by 2 articles
-
Comparison of Locking Compression Plate Superior Anterior Clavicle Plate with Suture Augmentation and Hook Plate for Treatment of Distal Clavicle Fractures
Jun-Cheol Choi, Woo-Suk Song, Woo-Sung Kim, Jeong-Muk Kim, Chan-Woong Byun
Arch Hand Microsurg. 2017;22(4):247-255. doi: 10.12790/ahm.2017.22.4.247.The Risk Factors Associated with Nonunion after Surgical Treatment for Distal Fibular Fractures
Jun Young Lee, Kwi Youn Choi, Sinwook Kang, Kang Yeol Ko
J Korean Foot Ankle Soc. 2018;22(3):95-99. doi: 10.14193/jkfas.2018.22.3.95.
Reference
-
1. Heppenstall RB. Fractures and dislocations of the distal clavicle. Orthop Clin North Am. 1975; 6:477–486.
Article2. Deafenbaugh MK, Dugdale TW, Staeheli JW, Nielsen R. Non-operative treatment of Neer type II distal clavicle fractures: a prospective study. Contemp Orthop. 1990; 20:405–413.3. Neer CS 2nd. Fracture of the distal clavicle with detachment of the coracoclavicular ligaments in adults. J Trauma. 1963; 3:99–110.
Article4. Neer CS 2nd. Fractures of the distal third of the clavicle. Clin Orthop Relat Res. 1968; 58:43–50.5. Nordqvist A, Petersson C, Redlund-Johnell I. The natural course of lateral clavicle fracture. 15 (11-21) year follow-up of 110 cases. Acta Orthop Scand. 1993; 64:87–91.
Article6. Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am. 2004; 86:1359–1365.
Article7. Rokito AS, Zuckerman JD, Shaari JM, Eisenberg DP, Cuomo F, Gallagher MA. A comparison of nonoperative and operative treatment of type II distal clavicle fractures. Bull Hosp Jt Dis. 2002-2003; 61:32–39.8. Banerjee R, Waterman B, Padalecki J, Robertson W. Management of distal clavicle fractures. J Am Acad Orthop Surg. 2011; 19:392–401.
Article9. Neviaser RJ. Injuries to the clavicle and acromioclavicular joint. Orthop Clin North Am. 1987; 18:433–438.
Article10. Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br. 1998; 80:476–484.11. Oh JH, Choi HY. Recent treatment options for the clavicle fracture. Clin Should Elbow. 2012; 15:43–51.
Article12. Anderson K. Evaluation and treatment of distal clavicle fractures. Clin Sports Med. 2003; 22:319–326. vii.
Article13. Hessmann M, Kirchner R, Baumgaertel F, Gehling H, Gotzen L. Treatment of unstable distal clavicular fractures with and without lesions of the acromioclavicular joint. Injury. 1996; 27:47–52.
Article14. Robinson CM, Cairns DA. Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am. 2004; 86-A:778–782.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current Concepts for Classification and Treatment of Distal Clavicle Fractures
- Conservative Treatment of Mid-Clavicle Fractures
- Current concepts in the treatment of midshaft clavicle fractures in adults
- Operative Treatment of Distal Clavicle Fracture Nonunion
- Periprosthetic Clavicle Shaft Fracture After Treatment of Type V Distal Clavicle Fracture Using a Hook Plate: A Report of Two Cases
