Pelvic Bone Fracture with Bladder Rupture
- Affiliations
-
- 1Department of Orthopaedic Surgery, School of Medicine, Chosun University, Gwangju, Korea. kkamtol@hanmail.net
- 2Department of Urology, School of Medicine, Chosun University, Gwangju, Korea.
- KMID: 2106676
- DOI: http://doi.org/10.4055/jkoa.2013.48.3.222
Abstract
- PURPOSE
The purpose of this study was to evaluate the injury mechanism of pelvic bone fracture and injury type and treatment of bladder rupture associated with pelvic bone fracture.
MATERIALS AND METHODS
From September 2002 to February 2011, we treated pelvic bone fracture with bladder rupture in 56 cases with minimal follow up of one year. Each of the 56 cases was classified into groups depending on the mechanism of pelvic fracture (Young classification) and the aspect of bladder rupture (intraperitoneal rupture, extraperitoneal rupture, combined rupture) after which the relationship between the two aspects was analyzed retrospectively.
RESULTS
There were a total of 56 cases where bladder ruptures occurred in association with pelvic bone fractures; 34 patients were men and 22 patients were women. The average age was 58.2 years (range: 19-84). Traffic accidents were the main cause of pelvic bone fractures with bladder ruptures in 41 cases. The main injury mechanism was lateral compression, and pubic ramus fractures occurred in 38 cases (67.9%). Regarding the classifications of bladder ruptures, there were 17 cases of intraperitoneal rupture, 37 cases of extraperitoneal rupture, and two cases of combined rupture. Operations were performed on all cases of intraperitoneal and combined rupture and on six cases of extraperitoneal rupture.
CONCLUSION
Lateral compression was the most common injury of bladder rupture in pelvic bone fracture. Bladder ruptures occurred even in cases where the displacement of pelvic bones was not severe and also in cases of low energy injury.
MeSH Terms
Figure
-
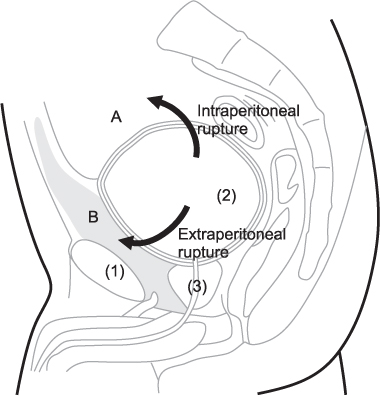
Figure 1 Rupture of the urinary bladder. A: intraperitoneal cavity, B: extraperitoneal cavity, (1) pubic ramus, (2) bladder, (3) urethra.

Figure 2 A 59-year-old female patient was injured after falling down, with occurrence of right pubic inferior ramus fracture, left sacral alar fracture, and sacroiliac joint separation (not classified by Young classification). (A) Pelvic inlet image shows bony fragments of the right pubic inferior ramus fracture (black arrow). (B) Pelvis computed tomography axial view shows bladder rupture by bony fragments of the pubic ramus (black arrow). (C) Cystogram shows extraperitoneal contrast material extravasation extending around the bladder (black arrows). This cystogram shows an extraperitoneal bladder rupture. (D) Clinical picture shows intraoperative finding that bladder ruptured by bony fragments of the pubic ramus. (E) Excision of bony fragments. (F) Cystogram shows a well-repaired bladder with no contrast leakage at two weeks after the operation.
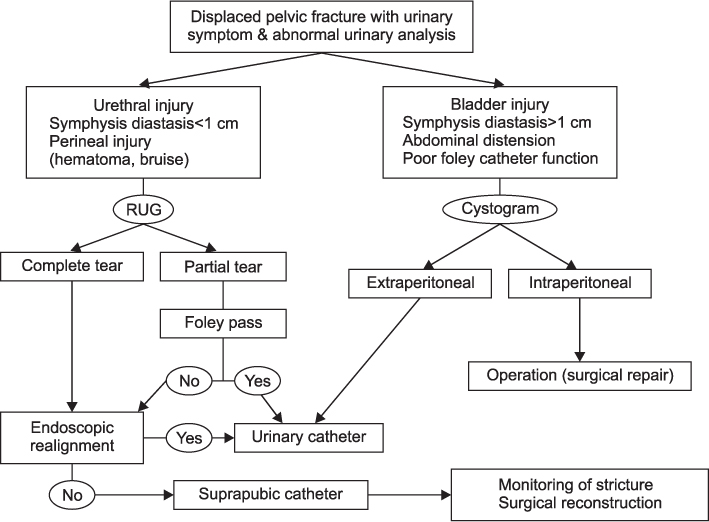
Figure 3 Algorithm for diagnosis and management of bladder and urethral injuries associated with pelvic fractures. RUG, retrograde urethrogram.

Figure 4 A 58-year-old male patient was injured after being pressed by a tree, with occurrence of right iliac wing comminuted fracture, both pubic superior and inferior ramus fracture, and right sacral alar fracture (lateral compression grade III injury of Young classification). (A) Cystogram shows extraperitoneal contrast material extravasation extending around the bladder (black arrows). This cystogram shows an extraperitoneal bladder rupture. (B) Retrograde urethrogram shows contrast material extravasation from the posterior urethra (black arrow). This retrograde urethrogram shows injury of the posterior urethra. (C) Cystogram shows a well-healing bladder, with no leakage of contrast material at two weeks after foley catheter insertion. (D) Retrograde urethrogram shows a well-healing posterior urethra, with no leakage of contrast material at two weeks after foley catheter insertion. (E) Retrograde urethrogram shows a well-healing posterior urethra without stricture at two months after Foley catheter insertion.
Reference
-
1. Wright DG, Taitsman L, Laughlin RT. Pelvic and bladder trauma: a case report and subject review. J Orthop Trauma. 1996; 10:351–354.2. Peltier LF. complications associated with fractures of the pelvis. J Bone Joint Surg Am. 1965; 47:1060–1069.
Article3. Antoci JP, Schiff M Jr. Bladder and urethral injuries in patients with pelvic fractures. J Urol. 1982; 128:25–26.
Article4. Hauschild O, Strohm PC, Culemann U, et al. Mortality in patients with pelvic fractures: results from the German pelvic injury register. J Trauma. 2008; 64:449–455.
Article5. Lynch TH, Martínez-Piñeiro L, Plas E, et al. European Association of Urology. EAU guidelines on urological trauma. Eur Urol. 2005; 47:1–15.
Article6. Young JW, Burgess AR, Brumback RJ, Poka A. Pelvic fractures: value of plain radiography in early assessment and management. Radiology. 1986; 160:445–451.
Article7. Belis JA, Recht KA, Milam DF. Simultaneous traumatic bladder perforation and disruption of the prostatomembranous urethra. J Urol. 1979; 122:412–414.
Article8. Pennal GF, Tile M, Waddell JP, Garside H. Pelvic disruption: assessment and classification. Clin Orthop Relat Res. 1980; 151:12–21.
Article9. Sandler CM, Hall JT, Rodriguez MB, Corriere JN Jr. Bladder injury in blunt pelvic trauma. Radiology. 1986; 158:633–638.
Article10. Pokorny M, Pontes JE, Pierce JM Jr. Urological injuries associated with pelvic trauma. J Urol. 1979; 121:455–457.
Article11. Corriere JN Jr, Sandler CM. Mechanisms of injury, patterns of extravasation and management of extraperitoneal bladder rupture due to blunt trauma. J Urol. 1988; 139:43–44.
Article12. Flaherty JJ, Kelley R, Burnett B, et al. Relationship of pelvic bone fracture patterns to injuries of urethra and bladder. J Urol. 1968; 99:297–300.
Article13. Bodner DR, Selzman AA, Spirnak JP. Evaluation and treatment of bladder rupture. Semin Urol. 1995; 13:62–65.14. Figler B, Hoffler CE, Reisman W, et al. Multi-disciplinary update on pelvic fracture associated bladder and urethral injuries. Injury. 2012; 43:1242–1249.
Article15. Gomez RG, Ceballos L, Coburn M, et al. Consensus statement on bladder injuries. BJU Int. 2004; 94:27–32.
Article16. Tile M. Pelvic ring fractures: should they be fixed? J Bone Joint Surg Br. 1988; 70:1–12.
Article17. Pavlov H, Nelson TL, Warren RF, Torg JS, Burstein AH. Stress fractures of the pubic ramus. A report of twelve cases. J Bone Joint Surg Am. 1982; 64:1020–1025.
Article18. Matta JM, Tornetta P 3rd. Internal fixation of unstable pelvic ring injuries. Clin Orthop Relat Res. 1996; 329:129–140.
Article19. Keating J. Delayed reconstruction of pelvic fractures. Curr Orthop. 2005; 19:362–372.20. Gruen GS, Leit ME, Gruen RJ, Garrison HG, Auble TE, Peitzman AB. Functional outcome of patients with unstable pelvic ring fractures stabilized with open reduction and internal fixation. J Trauma. 1995; 39:838–844.
Article21. Roumen RM, Hendriks T, van der Ven-Jongekrijg J, et al. Cytokine patterns in patients after major vascular surgery, hemorrhagic shock, and severe blunt trauma. Relation with subsequent adult respiratory distress syndrome and multiple organ failure. Ann Surg. 1993; 218:769–776.
Article22. Probst C, Probst T, Gaensslen A, Krettek C, Pape HC. Polytrauma Study Group of the German Trauma Society. Timing and duration of the initial pelvic stabilization after multiple trauma in patients from the German trauma registry: is there an influence on outcome? J Trauma. 2007; 62:370–377.
Article23. Hochberg E, Stone NN. Bladder rupture associated with pelvic fracture due to blunt trauma. Urology. 1993; 41:531–533.
Article24. Avey G, Blackmore CC, Wessells H, Wright JL, Talner LB. Radiographic and clinical predictors of bladder rupture in blunt trauma patients with pelvic fracture. Acad Radiol. 2006; 13:573–579.
Article25. Morgan DE, Nallamala LK, Kenney PJ, Mayo MS, Rue LW 3rd. CT cystography: radiographic and clinical predictors of bladder rupture. AJR Am J Roentgenol. 2000; 174:89–95.26. Parker H, Hoonpongsimanont W, Vaca F, Lotfipour S. Spontaneous bladder rupture in association with alcoholic binge: a case report and review of the literature. J Emerg Med. 2009; 37:386–389.
Article27. Festini G, Gregorutti S, Reina G, Bellis GB. Isolated intraperitoneal bladder rupture in patients with alcohol intoxication and minor abdominal trauma. Ann Emerg Med. 1991; 20:1371–1372.
Article28. Koraitim MM. Pelvic fracture urethral injuries: evaluation of various methods of management. J Urol. 1996; 156:1288–1291.
Article29. Wu XM. Concomitant rupture of bladder and posterior urethra in fracture of pelvis, analysis of 36 cases. Zhonghua Wai Ke Za Zhi. 1993; 31:663–665.30. Spirnak JP. Pelvic fracture and injury to the lower urinary tract. Surg Clin North Am. 1988; 68:1057–1069.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relationship of the patterns of pelvic bone fracture and bladder rupture
- Traumatic Bladder Rupture in Pelvic Fracture - Case Report
- Vesical and paravesical injuries: CT findings
- A roentgenographic study of the posterior urethral injury associated with pelvic bone fracture in male
- Delayed Presentation of Intravesical Bone Penetration after Pelvic Ring Fracture
