The Efficacy of Trochanteric Flip Osteotomy in Cases of Femoral Head Fracture
- Affiliations
-
- 1Department of Orthopedic Surgery, School of Medicine, Keimyung University, Daegu, Korea. min@dsmc.or.kr
- KMID: 2106674
- DOI: http://doi.org/10.4055/jkoa.2013.48.3.205
Abstract
- PURPOSE
The purpose of this study is to evaluate the clinical and radiological results of the trochanteric flip osteotomy in cases of femoral head fractures.
MATERIALS AND METHODS
Between May 2000 and January 2012, we evaluated 14 cases of femoral head fractures treated by trochanteric flip osteotomy in combination with the Kocher-Langenbeck approach after a minimum follow-up of one year. There were 13 men and one woman and the average follow-up period was 36.4 months. The clinical results were evaluated according to Merle d'Aubigne-Postel scores and the Thompson-Epstein scoring scale and the radiological results were evaluated according to time to union of fractures and osteotomy site. We also evaluated the incidence of complications.
RESULTS
At the last follow-up, mean Merle d'Aubigne-Postel score was 16.4 and 11 cases out of 14 patients presented with good to excellent, two cases presented with fair, and one case presented with a poor clinical result according to the Thompson-Epstein scoring scale. Radiologically all cases achieved union of fractures and osteotomy site and the mean time to union of the osteotomy site was 7.9 weeks. Complications included one case of heterotopic ossification which did not disturb hip function, two cases of avascular necrosis of the femoral head, and one case of post-traumatic osteoarthritis.
CONCLUSION
The trochanteric flip osteotomy in the case of a femoral head fracture showed good clinical and radiological results through good visualization and accurate reduction of the fracture site. However, conduct of further studies including larger number of patients is needed in order to evaluate the incidence of complications such as avascular necrosis of the femoral head.
Keyword
MeSH Terms
Figure
-
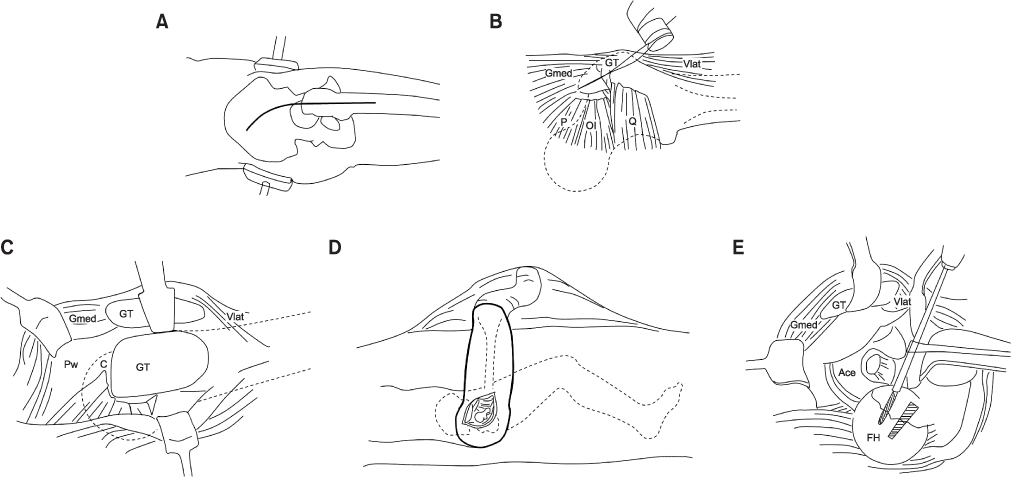
Figure 1 Diagram shows the surgical technique of the trochanteric flip osteotomy. (A) Patient lies in the lateral decubitus position on the operating table and the Kocher-Langenbeck approach is used. (B) As oscillating saw is used for the trochanteric flip osteotomy. The majority of the gluteus medius tendon is attached proximally and the insertion of the vastus lateralis muscle is attached distally at the fragment. (C) Exposure of the capsule and posterosuperior acetabular wall is achieved with anterior flipping of the osteotomized trochanteric fragment. (D) For dislocation of the femoral head, the hip is flexed, externally rotated, and the leg is brought over the front of the operating table and placed in a sterile bag. (E) After dislocation of the femoral head, the fracture can be easily visualized, reduced and stabilized. GT, greater trochanter; Gmed, gluteus medius; Vlat, vastus lateralis; P, piriformis muscle; OI, obturator internus; Q, quadratus femoris; Pw, posterosuperior acetabular wall; C, capsule; FH, femoral head; Ace, acetabulum.
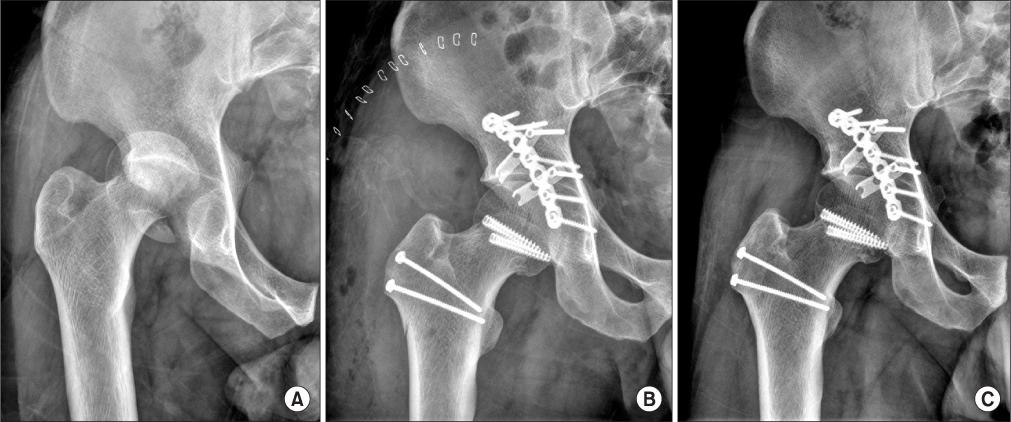
Figure 2 (A) Preoperative anteroposterior pelvic radiograph of a 33 year-old male shows the femoral head fracture of Pipkin type IV. (B) Postoperative radiograph shows an anatomic reduction and internal fixation with headless screws, spring plates. (C) Radiograph obtained at postoperative 23 months shows union of the fracture and osteotomy site. There is no evidence of avascular necrosis of the femoral head or posttraumatic osteoarthritis.
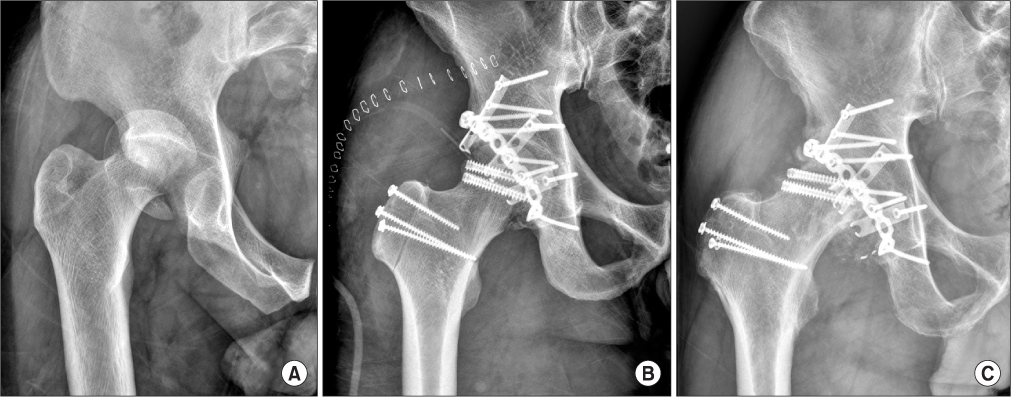
Figure 3 (A) Preoperative anteroposterior pelvic radiograph shows the femoral head fracture of Pipkin type IV. (B) Postoperative radiograph shows an anatomic reduction and internal fixation with headless screws, spring plates. (C) Radiograph obtained postoperative 34 months shows avascular necrosis of the femoral head.
Reference
-
1. Hougaard K, Thomsen PB. Traumatic posterior fracture-dislocation of the hip with fracture of the femoral head or neck, or both. J Bone Joint Surg Am. 1988; 70:233–239.
Article2. Lang-Stevenson A, Getty CJ. The Pipkin fracture-dislocation of the hip. Injury. 1987; 18:264–269.
Article3. Henle P, Kloen P, Siebenrock KA. Femoral head injuries: which treatment strategy can be recommended? Injury. 2007; 38:478–488.
Article4. Butler JE. Pipkin Type-II fractures of the femoral head. J Bone Joint Surg Am. 1981; 63:1292–1296.
Article5. Marchetti ME, Steinberg GG, Coumas JM. Intermediate-term experience of Pipkin fracture-dislocations of the hip. J Orthop Trauma. 1996; 10:455–461.
Article6. Letournel E, Judet R. Fractures of the acetabulum. 2nd ed. Berlin: Springer-Verlag;1993. p. 67–85. p. 323–327. p. 364–373. p. 417–421. p. 545–581.7. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am. 1996; 78:1632–1645.8. Bray TJ, Esser M, Fulkerson L. Osteotomy of the trochanter in open reduction and internal fixation of acetabular fractures. J Bone Joint Surg Am. 1987; 69:711–717.
Article9. Solberg BD, Moon CN, Franco DP. Use of a trochanteric flip osteotomy improves outcomes in Pipkin IV fractures. Clin Orthop Relat Res. 2009; 467:929–933.
Article10. Naranje S, Shamshery P, Yadav CS, Gupta V, Nag HL. Digastric trochanteric flip osteotomy and surgical dislocation of hip in the management of acetabular fractures. Arch Orthop Trauma Surg. 2010; 130:93–101.
Article11. Siebenrock KA, Gautier E, Ziran BH, Ganz R. Trochanteric flip osteotomy for cranial extension and muscle protection in acetabular fracture fixation using a Kocher-Langenbeck approach. J Orthop Trauma. 1998; 12:387–391.
Article12. Kim JW, Chang JS, Bae JY, Kim JJ. Outcomes of treatment for femoral head fractures with hip dislocation: review of 20 cases. J Korean Hip Soc. 2010; 22:298–304.13. Pipkin G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am. 1957; 39:1027–1042.
Article14. D'aubigne RM, Postel M. Functional results of hip arthroplasty with acrylic prosthesis. J Bone Joint Surg Am. 1954; 36:451–475.15. Thompson VP, Epstein HC. Traumatic dislocation of the hip; a survey of two hundred and four cases covering a period of twenty-one years. J Bone Joint Surg Am. 1951; 33:746–778.16. Epstein HC, Wiss DA, Cozen L. Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop Relat Res. 1985; 201:9–17.
Article17. Ganz R, Gill TJ, Gautier E, Ganz K, Krügel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001; 83:1119–1124.18. Mercati E, Guary A, Myguel C, Bourgeon A. A posteroexternal approach to the hip joint, Value of the formation of a digastric muscle. J Chir (Paris). 1972; 103:499–504.19. Siebenrock KA, Gautier E, Woo AK, Ganz R. Surgical dislocation of the femoral head for joint debridement and accurate reduction of fractures of the acetabulum. J Orthop Trauma. 2002; 16:543–552.
Article20. Brumback RJ, Kenzora JE, Levitt LE, Burgess AR, Poka A. Fractures of the femoral head. Hip. 1987; 181–206.21. Warren PJ. Fixation of a fracture of the femoral head with preservation of remaining soft-tissue attachments. J Orthop Trauma. 1991; 5:504–505.22. Nötzli HP, Siebenrock KA, Hempfing A, Ramseier LE, Ganz R. Perfusion of the femoral head during surgical dislocation of the hip. Monitoring by laser Doppler flowmetry. J Bone Joint Surg Br. 2002; 84:300–304.23. Daum WJ, Scarborough MT, Gordon W Jr, Uchida T. Heterotopic ossification and other perioperative complications of acetabular fractures. J Orthop Trauma. 1992; 6:427–432.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Subtrochanteric Femoral Fracture during Trochanteric Nailing for the Treatment of Femoral Shaft Fracture
- Preoperative Planning of Oblique Femoral Trochanteric Osteotomy by Geometric Analysis
- Posttraumatic Osteonecrosis of the Femoral Head after Nine Years of Posterior Femoral Head Fracture Dislocation
- Pseudoaneurysm of the Superficial Femoral Artery Following Gamma nail Fixation for Trochanteric Fracture: A Case Report
- A Clinical Observation of Hip Fractures
