Hip Morphometry of Femoroacetabular Impingement Pattern in Patients with Ankylosing Spondylitis
- Affiliations
-
- 1Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea. jachoi88@gmail.com
- 2Department of Radiology, Hallym University Dongtan Sacred Heart Hospital, Hwaseong, Korea.
- KMID: 2098017
- DOI: http://doi.org/10.3348/jksr.2015.72.6.385
Abstract
- PURPOSE
To analyze hip morphometry of femoroacetabular impingement (FAI) pattern in patients with ankylosing spondylitis (AS) and correlate them with sacroiliitis grades.
MATERIALS AND METHODS
384 patients with AS were analyzed regarding demographics, radiologic signs of FAI for hip involvement, and sacroiliitis grades. FAI was classified into 3 types according to alpha angle, lateral center-edge angle and pistol grip deformity. Sacroiliitis was graded according to the New York criteria. Prevalence of FAI morphometry types was determined and evaluated for association with sacroiliitis grades. Statistical analysis regarding numerical variables, including age, sacroiliitis score using t-test, sacroiliitis score in three groups using Kruskal-Wallis test and Mann-Whitney U-test, corrected by Bonferroni methods for post hoc analysis was done.
RESULTS
Among 384 patients, 141 (36.7%) had FAI morphometry. Male predominance was found in group with FAI pattern involvement (87.2%) (p = 0.000). Pincer type (20.6%) was the most common. Hip involvement group also showed greater sacroiliitis score (2.49 vs. 1.75, p = 0.000). Combined-type had greater sacroiliitis score compared with others (p = 0.002, 0.003).
CONCLUSION
FAI morphometry was frequent in hips of AS patients (36.7%), especially pincer type, more frequent in male, and associated with significantly greater grade of sacroiliitis; combined type FAI pattern had greater sacroiliitis score.
MeSH Terms
Figure
-

Fig. 1 Radiographic presentations of alpha angle on translateral radiograph by drawing a circle along the femur head circumference, drawing a line between the center of the circle and the point of head-neck offset, according to the method described by Nötzli et al. (6).
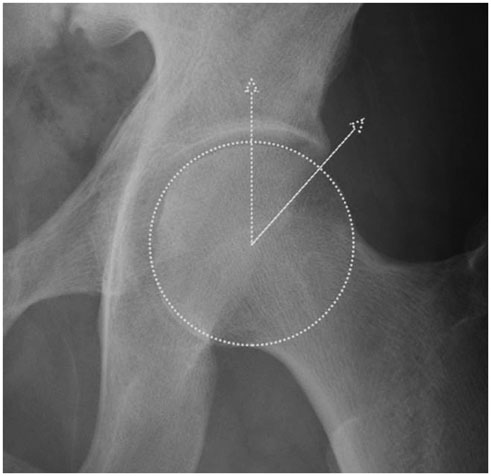
Fig. 2 Radiographic presentations of lateral center-edge angle on anteroposterior radiographs. The lateral center edge angle is the angle formed by a vertical line and a line connecting the femoral head center with the lateral edge of the acetabulum.
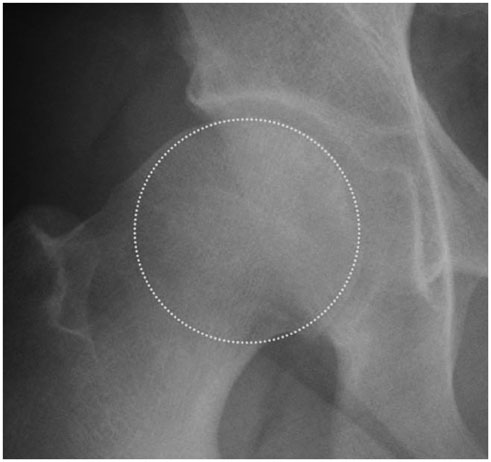
Fig. 3 Radiographic presentations of flattening of the head-neck junction (so called pistol grip deformity) on anteroposterior radiographs.

Fig. 4 Pelvic radiograph of 33-year-old man with ankylosing spondylitis. A. Pincer type femoroacetabular impingement pattern showing lateral center-edge angle estimated to be 52.3°. B. Demonstrating bilateral sacroiliitis grade 3, showing subchondral sclerosis and irregularities of the joint surface, including erosions.
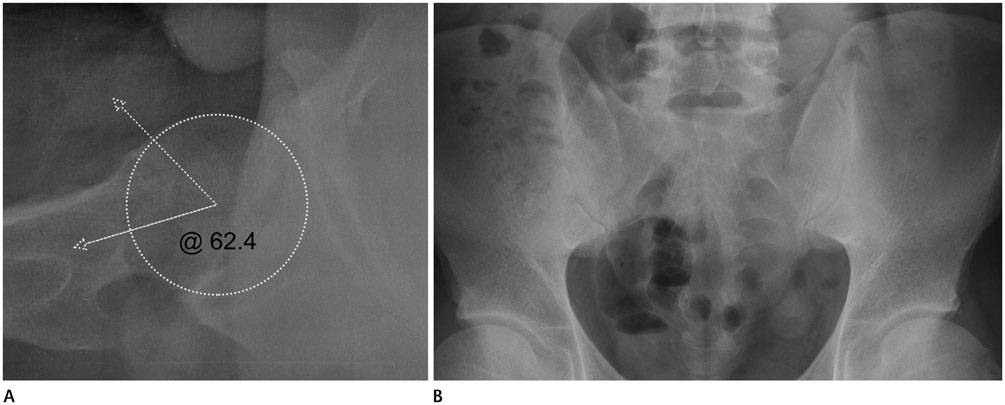
Fig. 5 Pelvic radiograph of in 26-year-old man with ankylosing spondylitis. A. Cam type femoroacetabular impingement pattern showing alpha angle estimated to be 62.4°. B. Demonstrating bilateral sacroiliitis grade 2, showing equivocal subchondral sclerosis.

Fig. 6 Pelvic radiograph of 31-year-old man with ankylosing spondylitis. A. Combined type femoroacetabular impingement pattern showing lateral center-edge angle estimated to be 45.0° and positive pistol grip deformity. B. Demonstrating bilateral sacroiliitis grade 4, showing complete ankylosis.
Reference
-
1. Baraliakos X, Braun J. Hip involvement in ankylosing spondylitis: what is the verdict? Rheumatology (Oxford). 2010; 49:3–3.2. Vander Cruyssen B, Muñoz-Gomariz E, Font P, Mulero J, de Vlam K, Boonen A, et al. Hip involvement in ankylosing spondylitis: epidemiology and risk factors associated with hip replacement surgery. Rheumatology (Oxford). 2010; 49:73–78.3. Tannast M, Siebenrock KA, Anderson SE. Femoroacetabular impingement: radiographic diagnosis--what the radiologist should know. AJR Am J Roentgenol. 2007; 188:1540–1552.4. Sutter R, Dietrich TJ, Zingg PO, Pfirrmann CW. Femoral antetorsion: comparing asymptomatic volunteers and patients with femoroacetabular impingement. Radiology. 2012; 263:475–483.5. Hack K, Di Primio G, Rakhra K, Beaulé PE. Prevalence of cam-type femoroacetabular impingement morphology in asymptomatic volunteers. J Bone Joint Surg Am. 2010; 92:2436–2444.6. Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002; 84:556–560.7. Pfirrmann CW, Mengiardi B, Dora C, Kalberer F, Zanetti M, Hodler J. Cam and pincer femoroacetabular impingement: characteristic MR arthrographic findings in 50 patients. Radiology. 2006; 240:778–785.8. Murphy SB, Kijewski PK, Millis MB, Harless A. Acetabular dysplasia in the adolescent and young adult. Clin Orthop Relat Res. 1990; (261):214–223.9. Tannast M, Siebenrock KA, Anderson SE. [Femoroacetabular impingement: radiographic diagnosis--what the radiologist should know]. Radiologia. 2008; 50:271–284.10. Murphy SB, Ganz R, Müller ME. The prognosis in untreated dysplasia of the hip. A study of radiographic factors that predict the outcome. J Bone Joint Surg Am. 1995; 77:985–998.11. Tönnis D, Heinecke A. Acetabular and femoral anteversion: relationship with osteoarthritis of the hip. J Bone Joint Surg Am. 1999; 81:1747–1770.12. Gran JT, Skomsvoll JF. The outcome of ankylosing spondylitis: a study of 100 patients. Br J Rheumatol. 1997; 36:766–771.13. Robertson LP, Davis MJ. A longitudinal study of disease activity and functional status in a hospital cohort of patients with ankylosing spondylitis. Rheumatology (Oxford). 2004; 43:1565–1156.14. Leunig M, Beck M, Dora C, Ganz R. [Femoroacetabular impingement: trigger for the development of coxarthrosis]. Orthopade. 2006; 35:77–84.15. Chakraverty JK, Sullivan C, Gan C, Narayanaswamy S, Kamath S. Cam and pincer femoroacetabular impingement: CT findings of features resembling femoroacetabular impingement in a young population without symptoms. AJR Am J Roentgenol. 2013; 200:389–395.16. Takeyama A, Naito M, Shiramizu K, Kiyama T. Prevalence of femoroacetabular impingement in Asian patients with osteoarthritis of the hip. Int Orthop. 2009; 33:1229–1232.17. Dodds MK, McCormack D, Mulhall KJ. Femoroacetabular impingement after slipped capital femoral epiphysis: does slip severity predict clinical symptoms? J Pediatr Orthop. 2009; 29:535–539.18. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005; 87:1012–1018.19. McBride MT, Muldoon MP, Santore RF, Trousdale RT, Wenger DR. Protrusio acetabuli: diagnosis and treatment. J Am Acad Orthop Surg. 2001; 9:79–88.20. Doran MF, Brophy S, MacKay K, Taylor G, Calin A. Predictors of longterm outcome in ankylosing spondylitis. J Rheumatol. 2003; 30:316–320.21. Brophy S, Mackay K, Al-Saidi A, Taylor G, Calin A. The natural history of ankylosing spondylitis as defined by radiological progression. J Rheumatol. 2002; 29:1236–1243.22. Brophy S, Calin A. Ankylosing spondylitis: interaction between genes, joints, age at onset, and disease expression. J Rheumatol. 2001; 28:2283–2288.23. Sampaio-Barros PD, Bertolo MB, Kraemer MH, Neto JF, Samara AM. Primary ankylosing spondylitis: patterns of disease in a Brazilian population of 147 patients. J Rheumatol. 2001; 28:560–565.24. Hickman JM, Peters CL. Hip pain in the young adult: diagnosis and treatment of disorders of the acetabular labrum and acetabular dysplasia. Am J Orthop (Belle Mead NJ). 2001; 30:459–446.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Efficacy of Intra-articular Steroid Injection in Patients with Femoroacetabular Impingement
- A Case of Ischiofemoral Impingement Syndrome as a Differential Diagnosis of Ankylosing Spondylitis
- Etanercept Treatment in Ankylosing Spondylitis Hip Lesions
- Controversial Issues in Arthroscopic Surgery for Femoroacetabular Impingement
- Femoroacetabular Impingement Syndrome
