Islet Cell Tumors of the Pancreas: A Variety of MultiphaseDynamic Imaging Findings with Pathologic Correlations Focusing on Nonfunctioning Tumors and Insulinomas
- Affiliations
-
- 1Department of Diagnostic Radiology, Gangnam Severance Hospital,Yonsei University College of Medicine, Korea. yjsrad97@yuhs.ac
- 2Department of Pathology, Gangnam Severance Hospital, Yonsei University College of Medicine, Korea.
- KMID: 2097919
- DOI: http://doi.org/10.3348/jksr.2010.63.5.463
Abstract
- Islet cell tumors (ICTs) are rare pancreatic neoplasms of neuroendocrine origin, posing a diagnostic challenge to radiologists. We illustrated a spectrum of features of pancreatic ICTs that could be found on multiphase dynamic CT or MRI, and elucidated the histopathologic characteristics by determining the contrast enhancement pattern of the lesions. Various enhancement patterns were dependant on the internal composition of the tumor, that is, the proportion of vascular densities for early enhancement and non-hypervascular interstitial tissue for late enhancement regardless of the size or functional behavior. This knowledge of the imaging-pathologic spectrum of ICTs could be helpful for the proper differential diagnosis from other pancreatic tumors.
MeSH Terms
Figure
-
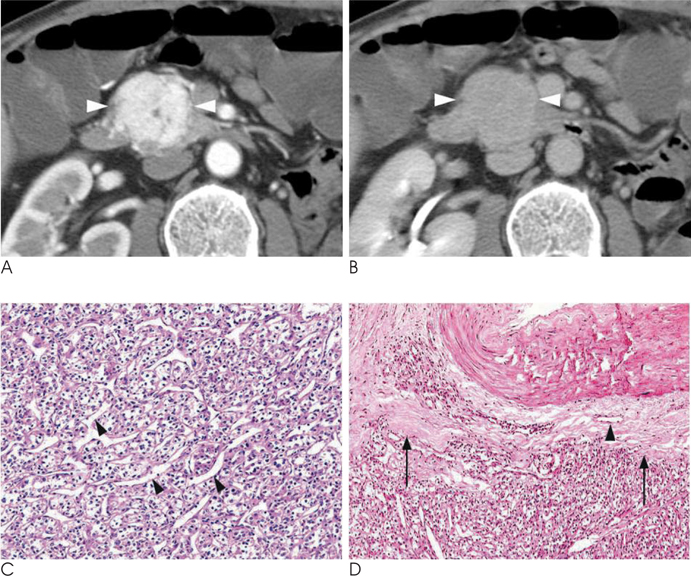
Fig. 1 A 70-year-old man with a nonfunctioning islet cell tumor that was found incidentally. A. A transverse contrast-enhanced CT scan obtained during the arterial phase shows a 3.8 cm, revealed a relatively homogeneous, strongly enhancing mass in the head portion of pancreas (arrowheads). B. A delayed phase image at the same level as A, showed a markedly decreased attenuation density in the lesion (arrowheads), which is similar to or slightly lower than the intraluminal densities of adjacent vasculatures. C. A photomicrograph (original magnification × 200, hematoxylin-eosin stain) showed tumor cells with abundant intervening vascular sinusoids (arrowheads). D. A small vascular structure (arrowhead) in the irregular fibrotic capsule (arrows) was demonstrated. The lesion consists mostly of abundant tumor cells, intervening sinusoids, and scanty fibrotic interstitial space on the photomicrograph (original magnification × 100, hematoxylin-eosin stain).
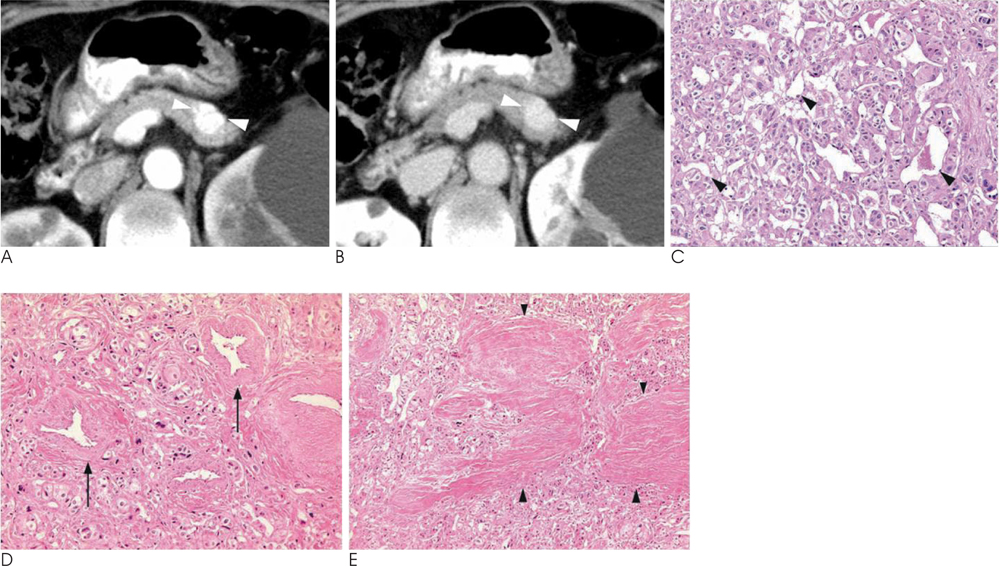
Fig. 2 A 64-year-old woman with functioning insulinoma. A. Transverse contrast-enhanced CT scan obtained during the arterial phase showed a 1.5 cm homogeneously and strongly enhancing, lobulated mass in the body-tail portion of pancreas (arrowheads). B. A delayed phase image at the same level as A, showed a sustained contrast enhancement in the lesion (arrowheads). C. A photomicrograph (original magnification × 200, hematoxylin-eosin stain) showed tumor cells with abundant, variably-sized and intervening vascular sinusoids (arrowheads) in the lesion. D. Numerous intratumoral thick-walled arterial vasculatures (arrows) were prominently demonstrated on the photomicrograph (original magnification × 200, hematoxylin-eosin stain). Many arterial tumor feeding vessels were also noted in the fibrotic capsule (not shown). E. Tumoral parenchyma was also found to contain abundant irregular thick fibrous components with sclerotic hyalinized stroma (arrowheads) on the photomicrograph (original magnification × 100, hematoxylin-eosin stain).
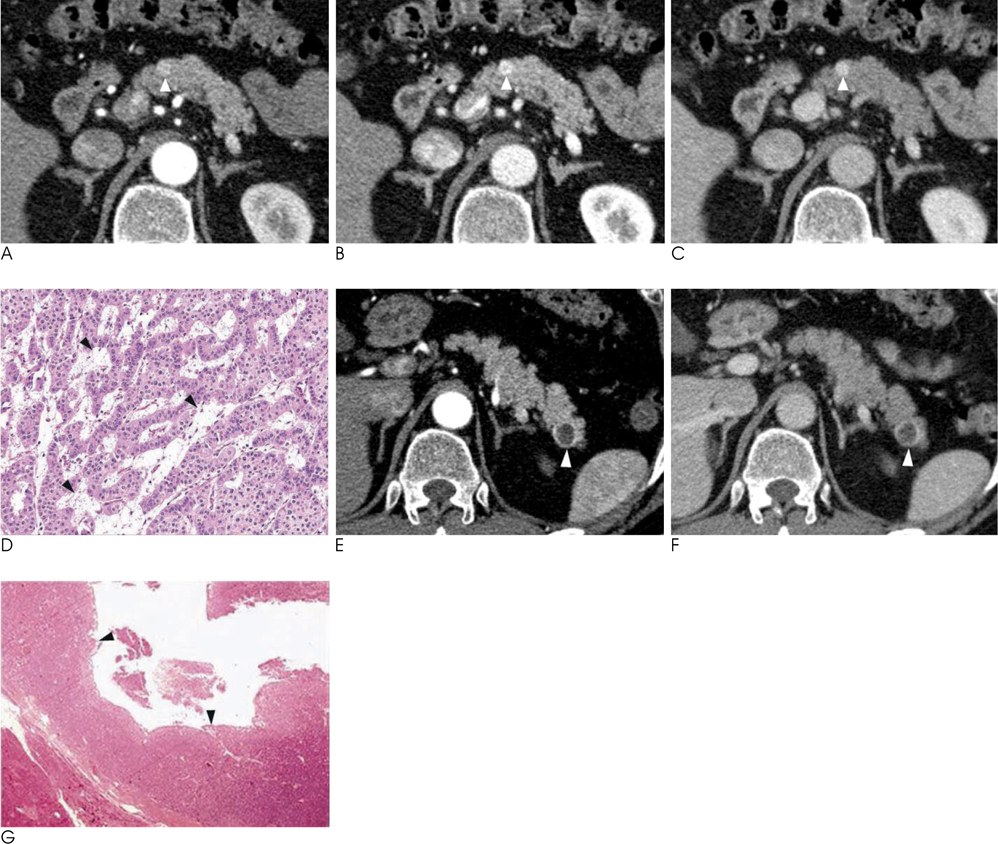
Fig. 3 A 48-year-old man with multiple, small, well enhancing insulinomas with lagged peak enhancement. A. On the transverse CT scan of the arterial phase, a 0.7 cm small nodular lesion on the body portion showed slight enhancement (arrowhead). B. The pancreatic body lesion was more prominently found with strong enhancement (arrowhead) on the portal phase images of dynamic CT. C. Prominent contrast enhancement was still present (arrowhead) during the equilibrium phase of the post-contrast CT. D. A photomicrograph (original magnification ×200, hematoxylin-eosin stain) of the solid lesion shows tumor cells with abundant intervening interstitial spaces of loose fibrotic connective tissue. Several small capillary vessels (arrowheads) were scattered in the connective tissue stroma without prominent sinusoidal vascular spaces. E. An early phase image of a post-contrast CT scan showed a 1.3 cm cystic lesion surrounded by a thin enhancing wall (arrowhead) in the tail of the pancreas. F. The pancreatic tail lesion still showed a non-enhancing cystic component surrounded by an enhancing wall (arrowhead) on the equilibrium phase imaging (Reprinted with permission from Lippincott Williams & Wilkins). G. A photomicrograph (original magnification × 20, hematoxylin-eosin stain) of the cystic lesion showed a cystic space lined by tumorous islet cells.
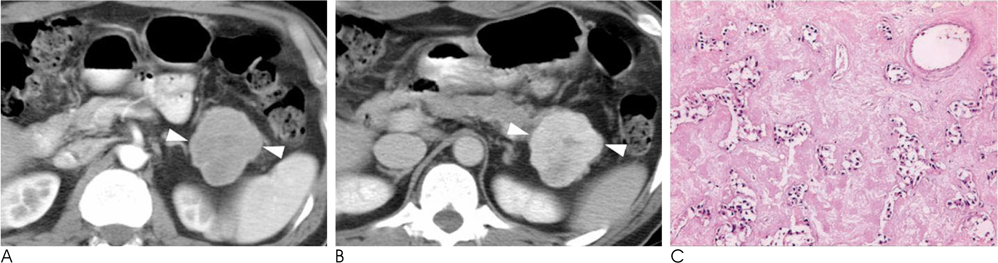
Fig. 4 A 46-year-old man with an incidentally found nonfunctioning islet cell tumor showed gradual and delayed contrast enhancement during a dynamic CT examination. A. A post-contrast CT scan obtained during the arterial dominant phase shows a 5 cm well-defined, marginally-enhancing and lobulated mass (arrowheads) in the tail of the pancreas. On the pre-contrast images, the mass demonstrated isoattenuation with the adjacent pancreatic tissue (not shown). B. On three-minute- delayed-phase CT, markedly higher attenuation density of the mass (arrowheads) permitted the lesion to be well distinguished from the remaining pancreatic parenchyma. C. The mass is mostly composed of amorphous sclerotic stroma with scanty tumor cells (arrow) on photomicrograph (original magnification × 200, hematoxylin-eosin stain). On Congo-red staining, the mass was hyalinized amyloid stroma (80%), showing birefringence (not shown).

Fig. 5 A 59-year-old man with abdominal pain and jaundice showed a malignant islet cell tumor mimicking a ductal cell adenocarcinoma in the tail of pancreas. A. On the transverse arterial phase dynamic CT scan, the poorly defined hypovascular lesion (arrowheads) in the tail of pancreas was found to be associated with a retracted contour of pancreatic parenchyma and direct invasion of the splenic vein. Hepatic metastasis showed a relatively high attenuation density due to the low attenuation of background hepatic parenchyma with diffuse fatty infiltration (arrow). B. Portal phase dynamic CT showed slight enhancement of the pancreatic lesion (arrowheads) with direct invasion of the splenic vein. Ring-like peripheral enhancement of the hepatic lesion (arrow) was also noted. C. Three-minute-delayed post-contrast CT showed a greater attenuation density of the primary pancreatic lesion with marginal spiculations, suggesting invasive tumor growth (arrowheads). D, E. A photomicrograph (original magnification × 200; D, hematoxylin-eosin stain; E, trichrome staining) of a sonography-guided liver biopsy specimen shows metastastic pancreatic endocrine tumor cells with abundant intervening thick collagenous bands (arrows).

Fig. 6 A 53-year-old man with a nonfunctioning islet cell tumor in the tail of the pancreas showed marked intratumoral hemorrhage mimicking a complicated cystic neoplasm. A. A T1-weighted transverse MRI illustrated intermediate signal intensity of the lesion surrounded by a hypointense fibrotic wall (arrowheads). Hypointense multiseptations were also defined within the lesion. B. A fat-suppressed T2-weighted MRI demonstrated a relatively homogeneous and hyperintense internal component with hypointense septa and an outer wall (arrowheads). C, D. An arterial phase (C) and equilibrium phase (D) dynamic MRI showed the contrast enhancement of intralesional septa (arrowheads). E. A photomicrograph (original magnification × 200, hematoxylin-eosin stain) showed scanty cellular islands separated by blood-filled stroma, suggesting the presence of conspicuous intratumoral hemorrhage. F. Markedly-dilated thick- and thin-walled vascular structures were filled with blood clots (arrows), suggesting severe intratumoral congestion on the photomicrograph (original magnification × 100, hematoxylin-eosins).
Reference
-
1. Eriguchi N, Aoyagi S, Hara M, Fukuda S, Tanaka E, Hashimoto M. Nonfunctioning islet cell carcinoma of the pancreas: an evaluation of seven patients who underwent resection followed by long-term survival. Surg Today. 1999; 29:233–237.2. Procacci C, Carbognin G, Accordini S, Biasiutti C, Bicego E, Romano L, et al. Nonfunctioning endocrine tumors of the pancreas: possibilities of spiral CT characterization. Eur Radiol. 2001; 11:1175–1183.3. Sheth S, Hruban RK, Fishman EK. Helical CT of islet cell tumors of the pancreas: typical and atypical manifestations. AJR Am J Roentgenol. 2002; 179:725–730.4. Rodallec M, Vilgrain V, Couvelard A, Rufat P, O'Toole D, Barrau V, et al. Endocrine pancreatic tumours and helical CT: contrast enhancement is correlated with microvascular density, histoprognostic factors and survival. Pancreatology. 2006; 6:77–85.5. McAuley G, Delaney H, Colville J, Lyburn L, Worsley D, Govender P, et al. Multimodality preoperative imaging of pancreatic insulinomas. Clin Radiol. 2005; 60:1039–1050.6. d'Assignies G, Couvelard A, Bahrami S, Vullierme MP, Hammel P, Hentic O, et al. Pancreatic endocrine tumors: tumor blood flow assessed with perfusion CT reflects angiogenesis and correlates with prognostic factors. Radiology. 2009; 250:407–416.7. Ichikawa T, Peterson MS, Federle MP, Baron RL, Haradome H, Kawamori Y, et al. Islet cell tumor of the pancreas: biphasic CT versus MR imaging in tumor detection. Radiology. 2000; 216:163–171.8. Iglesias A, Arias M, Casal M, Páramo C, Fiaño C, Brasa J. Unusual presentation of a pancreatic insulinoma in helical CT and dynamic contrast-enhanced MR imaging: case report. Eur Radiol. 2001; 11:926–930.9. Itai Y, Ohtomo K, Kokubo T, Yamauchi T, Minami M, Yashiro N, et al. CT of hepatic masses: significance of prolonged and delayed enhancement. AJR Am J Roentgenol. 1986; 146:729–733.10. Park MS, Kim KH, Lim JS, Lee JH, Kim JH, Kim SY, et al. Unusual cystic neoplasms in the pancreas: radiologic-pathologic correlation. J Comput Assist Tomogr. 2005; 29:610–616.
