Epidermoid Cyst of the Conus Medullaris and Cauda Equina: A case report
- Affiliations
-
- 1Department of Orthopaedic Surgery, Sun General Hospital, Daejeon, Korea. msmoonos@hotmail.com
- 2Department of Orthopaedic Surgery, Samsung Policlinic Center, Jeonju, Korea.
- KMID: 2097832
- DOI: http://doi.org/10.4184/jkss.2006.13.2.142
Abstract
- The objective of this study is to report on a case of a huge epidermoid cyst in the conus medullaris and cauda equina in a 43 year-old lady with the characteristic MRI and histologic findings. She suffered from low back pain, hypoesthesia around the anus and urinary incontinence for over 20 years. Since 15 years previously, she gradually developed right foot drop and muscle atrophy. She underwent surgery and unfortunately, she developed complete paralysis below T12 after complete tumor excision. At postoperative 4 weeks, evidence of partial neurological recovery down to the L3 roots was observed, but as yet there has been no further neurological recovery. Although total surgical excision is thought to be the only radical treatment, we recommend partial tumor excision to avoid damaging the spinal cord and cauda equina during the surgical procedure, than the radical excision, because this cyst is a very slowly growing benign tumor.
Keyword
MeSH Terms
Figure
-

Fig. 1. MRI finding of lumbar spine (A) Cystic segmented mass with hyperintense signal area in T1 weighted image and heterogeneous mass with hypointensity occupies the conus and the cauda equine from the T12 to L2. (B) Tumor mass occupies the almost entire canal, and the uninvolved root is extremely displaced to left side in axial views.

Fig. 2. Operative Findings : Huge irregularly shaped nodular tumor mass wall is seen, when the dura was open.
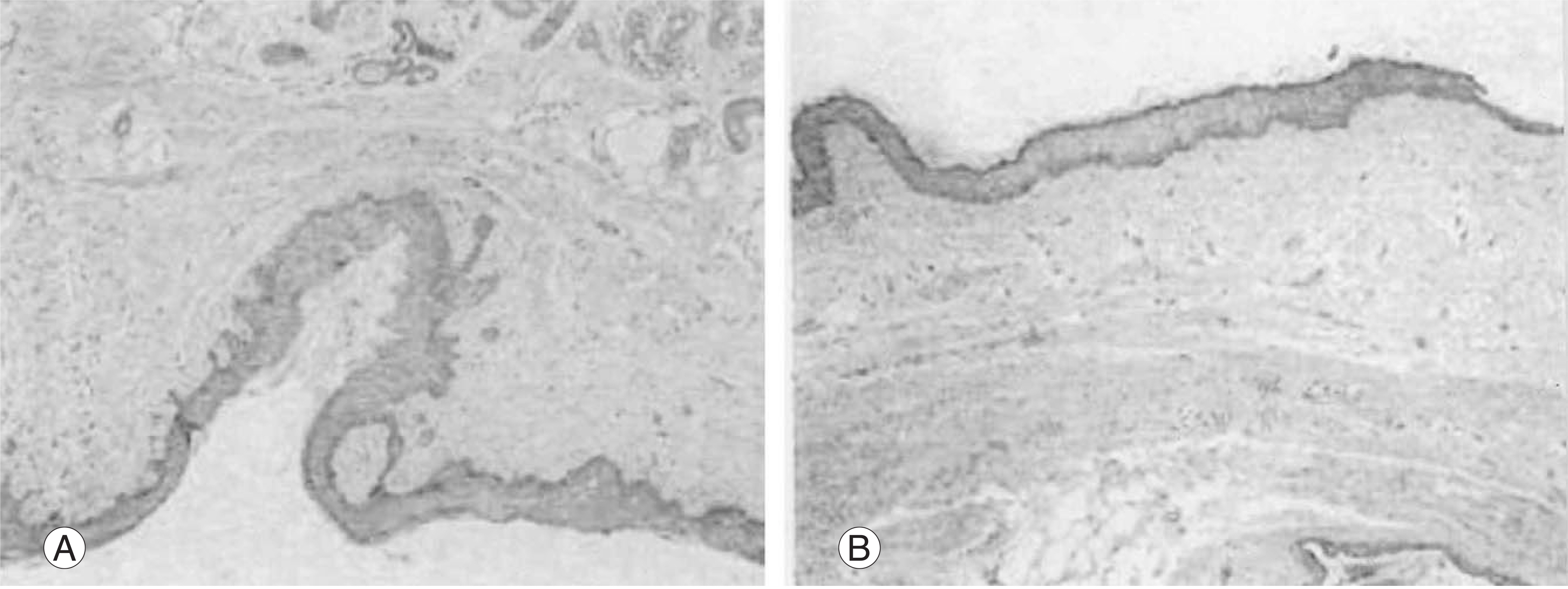
Fig. 3. (A) The microscopic finding shows keratin laid down by the well-developed squamous epithelium. The stroma reveals abun-dant skin appendages (100). But no sweat gland and hair follicles are seen. (B) The well-developed squamous epithelia are shown. The underlying stroma demonstrates loose mesenchymal tissue(X100).
Reference
-
01). Kim KJ., Shin BJ., Park JY., Yun TK., Kim YI. Intradur-al epidermoid cyst (in Korean): A case report. J. Korean Spine Surg. 7(3):401–405. 2000.02). Matsui H., Kanamori M., Yudoh K., Ohmori K., Yasude T., Wakaki K. Cystic spinal cord tumors: magnetic resonance imaging correlated to histopathological findings. Neurosurg. Rev. 21:147–151. 1998.03). Manno NJ., Uihlein A., Kernohan JW. Intraspinal epidermoids. J. Neurosurg. 19:754–765. 1962.04). Alves AM., Norrell H. Intramedullary epidermoid tumors of the spinal cord. Report of a case and review of the liter-ature. Int. Surg. 54:239–243. 1970.05). Roux A., Mercier C., Larbrisseau A., Dube LJ., Dupuis C., Del Carpio R. Intramedullary epidermoid cyst of the spinal cord. J. Neurosurg. 76:528–533. 1992.06). Phillip J., Chiu L. Magnetic resonance imaging of intraspinal epidermoid cyst: a case report. J. Comput. Assist Tomogr. 11:181–183. 1987.07). Graham DV., Tampieri D., Villemure JG. Intramedullary dermoid tumor diagnosed with the assistance of magnetic resonance imaging. Neurosurgery. 23:765–767. 1988.
Article08). Hatfield MK., Udesky RH., Strimling AM., Kim BH., Sibergleit R. MR imaging of a spinal epidermoid tumor. AJ NR,. 10:95–96. 1989.09). Russel DS., Rubinstein LJ. Pathology of tumors of the nervous system. Williams and Wilkins: Baltimore;1989.10). Gualdi GF., Di Biasi C., Trasimeni G., Pingi A., Vignati A., Maira G. Unusual MR and CT appearance of an epidermoid tumor. AJNR. 12:771–772. 1991.11). Lai SW., Chan WP., Chen CY., Chien JC., Chu JS., Chiu WT. MRI of epidermoid cyst of the conus medullaris: Care report. Spinal cord. 43:320–323. 2005.12). Horowitz BL., Chari MV., James R., Bryan RN. MR of intracranial epidermoid tumors: Correlation of in vivo imaging with in vitro C13 spectroscopy. AJNR. 11:299–302. 1990.13). Debray MP., Ricolfi F., Brugieres P., Khalil A., Adle-Biassette H., Gaston A. Epidermoid cyst of the conus medullaris; atypical MRI and angiographic features. Neuroradilegy. 38:526–528. 1996.
Article14). Dunn RC Jr., Archer CA., Rapport RL., Looi LM. Unusual CT-dense posterior fossa epidermoid cyst. Case report. J. Neurosurg. 55:654–656. 1981.15). Kim CK., Lee SG., Hwang S., Hong JK., Park JK. Lum-bar epidermoid inclusion cyst after single spinal pureture - A case report (in Korean). J. Korean Spine Surg. 7(2):271–275. 2000.16). Visciani A., Savoiardo M., Balestrini MR., Solero CL. Iatrogenic intraspinal epidermoid tumor: myelo-CT and MRI diagnosis. Neuroradiology. 31:273–275. 1989.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intradural Epidermoid Cyst at Conus Medullaris and Cauda Equina of the Spine: A Case Report
- Multiple Hemangioendotheliomas of the Spinal Cord and Cauda Equina: Case Report
- Multiple Intramedullary and Intradural Epidermoid Cysts in the Conus Medullaris and the Lumbar Spine: Case Report
- A Case of Dermoid in the Thoracolumbar Region
- Isolated Conus Medullaris Infarction: Rare Cases Highlighting Diagnostic Challenges and Clinical Insights
