Surgical Techniques for Repairing Foveal Tear of the Triangular Fibrocartilage Complex: Arthroscopic Transosseous Repair
- Affiliations
-
- 1Department of Orthopedic Surgery, Korea University College of Medicine, Seoul, Korea. ospark@korea.ac.kr
- KMID: 2097615
- DOI: http://doi.org/10.12790/jkssh.2014.19.2.95
Abstract
- As the importance of the foveal attachment of the triangular fibrocartilage complex (TFCC) on the stability of the distal radioulnar joint (DRUJ) is emphasized, the traditional repair techniques such as arthroscopic capsular repair for the 1B TFCC tear become accepted as ineffective method for treating DRUJ instability. Recently, several techniques which repair the TFCC directly to the ulnar fovea have been developed and introduced. Further advances of the techniques will be expected with increasing knowledge of the anatomy and biomechanics of the TFCC and DRUJ. Regardless of the techniques, fundamental principle of anatomical repair of the TFCC to the ulnar fovea is utmost important. Herein we present our technique of arthroscopic transosseous repair by making a drill hole in the ulnar and securing the sutures with Pushlock anchors.
MeSH Terms
Figure
-
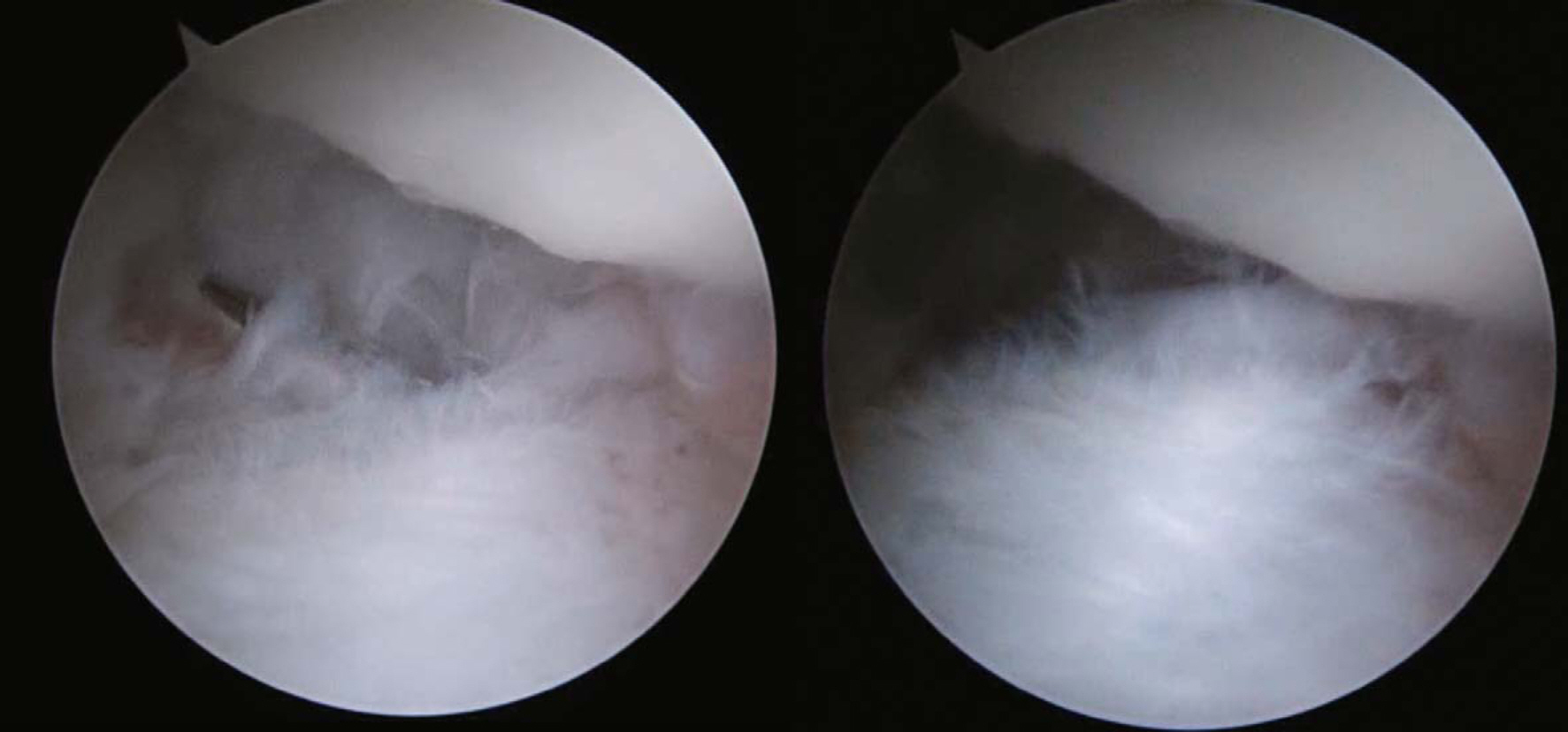
Fig. 1. Positive hook test indicates 1B pc-TFCC foveal attach tear. TFCC, triangular fibrocartilage complex.

Fig. 2. TFCC guide is helpful to make a transosseous tunnel at isometric poistion. TFCC, triangular fibrocartilage complex.
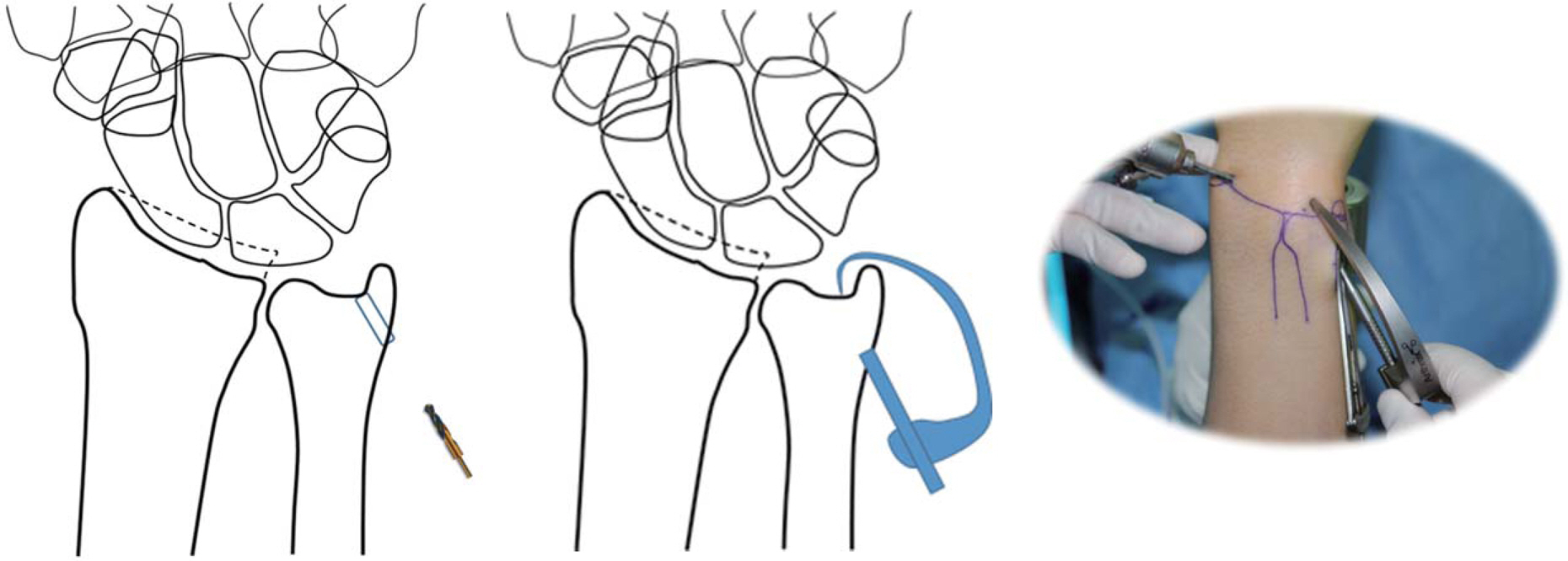
Fig. 3. 2.7 mm cannulated drilling for initial drilling. A TFCC guide is helpful to make transosseous tunnel at accurate position. TFCC, triangular fibrocartilage complex.
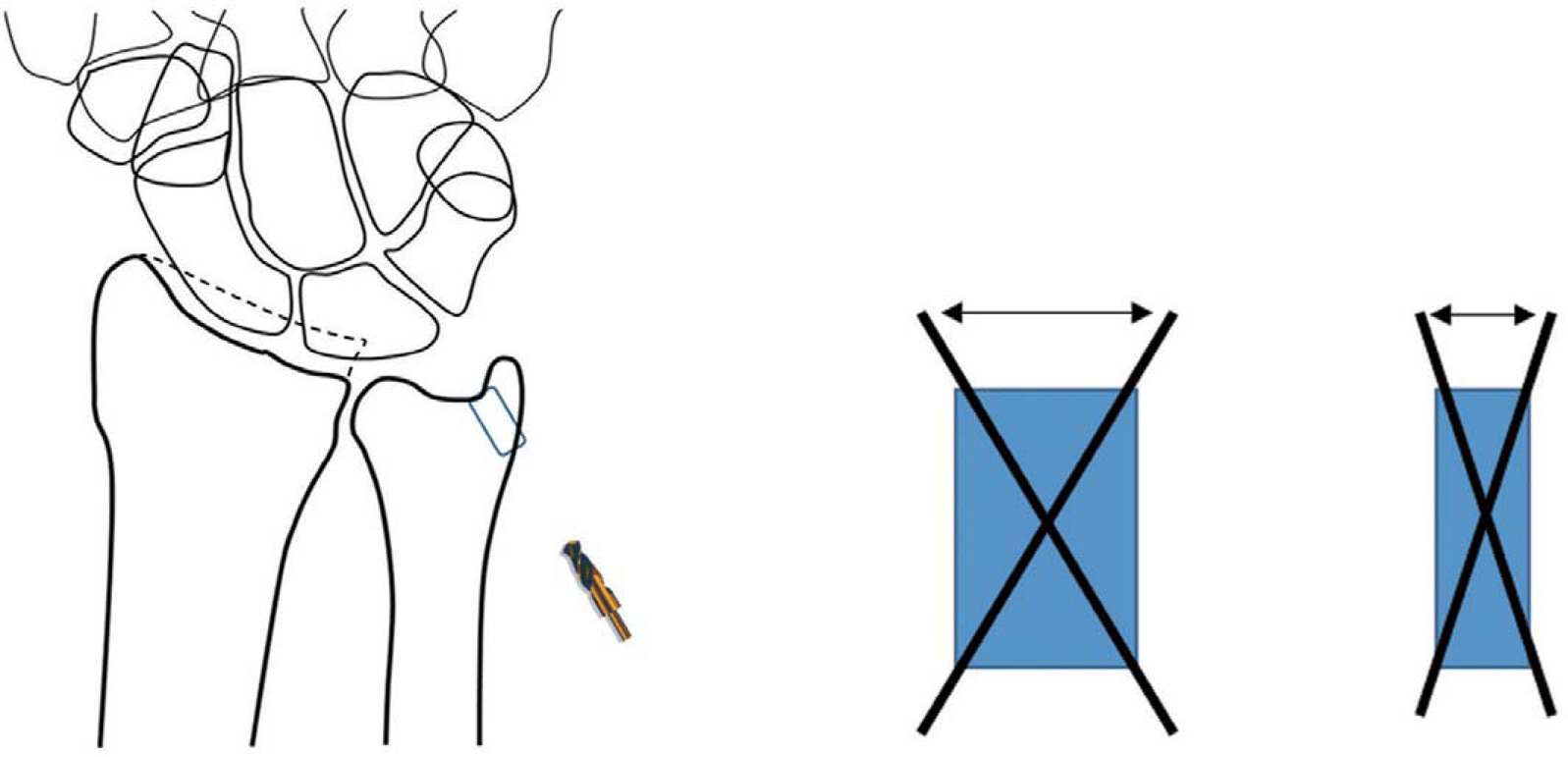
Fig. 4. 4 mm drilling provides more space for stable fixation.

Fig. 5. A bent fiberwire at needle tip prevents pull-out of suture from the joint when the needle is pulled-back from the bone tunnel.
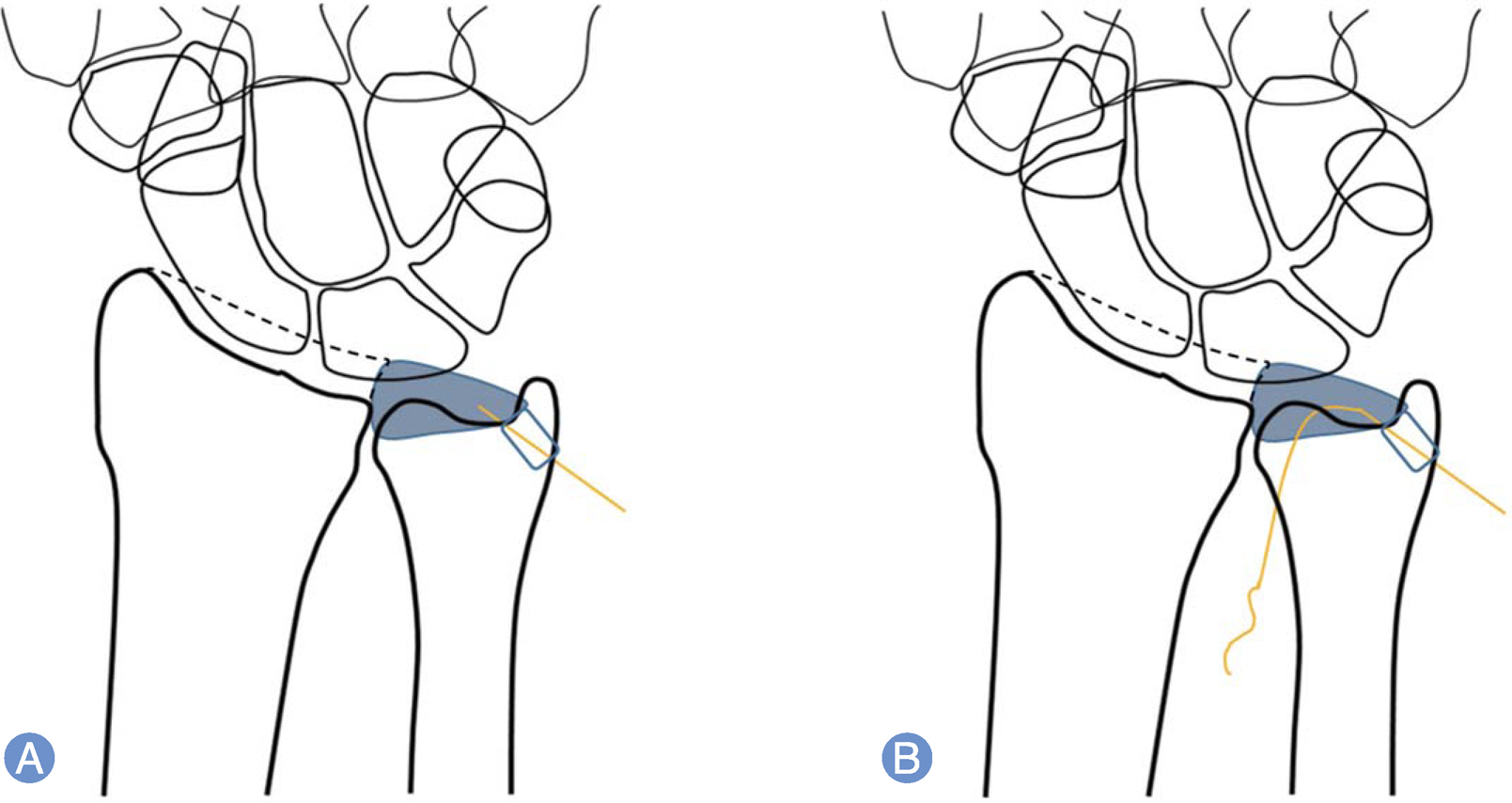
Fig. 6. (A, B) Fiberwire suture is pulled-out through the 8-R portal.

Fig. 7. A nitinol looped wire is passed through the 18-gauge needle.
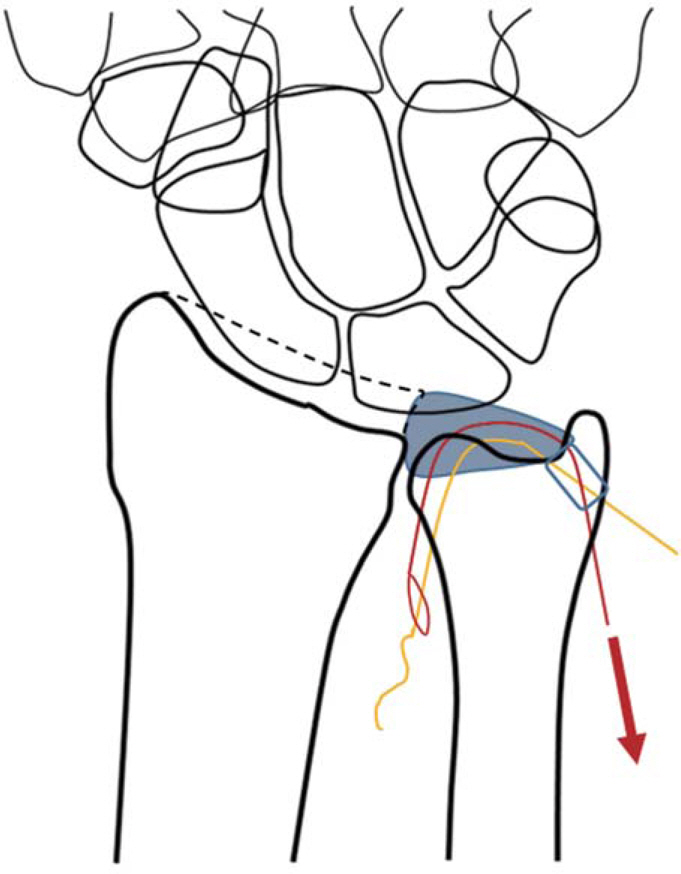
Fig. 8. The fiber wire is passed through the looped wire and pulled-back through the bone tunnel.

Fig. 9. (A, B) FIberwire is securely fixed with Pushlock.
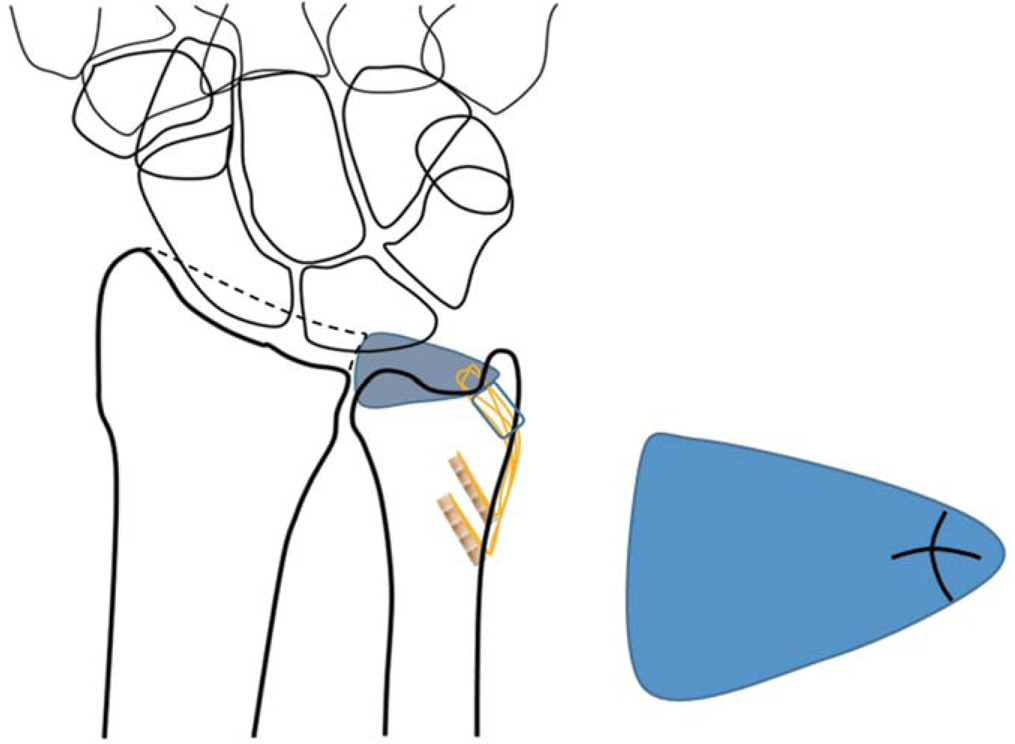
Fig. 10. Additional suture with cross configuration adds stability.
Reference
-
References
1. Atzei A, Rizzo A, Luchetti R, Fairplay T. Arthroscopic foveal repair of triangular fibrocartilage complex peripheral lesion with distal radioulnar joint instability. Tech Hand Up Extrem Surg. 2008; 12:226–35.
Article2. Lindau T, Adlercreutz C, Aspenberg P. Peripheral tears of the triangular fibrocartilage complex cause distal radioulnar joint instability after distal radial fractures. J Hand Surg Am. 2000; 25:464–8.
Article3. Millants P, De Smet L, Van Ransbeeck H. Outcome study of arthroscopic suturing of ulnar avulsions of the triangular fibrocartilage complex of the wrist. Chir Main. 2002; 21:298–300.
Article4. Nakamura T, Makita A. The proximal ligamentous component of the triangular fibrocartilage complex. J Hand Surg Br. 2000; 25:479–86.
Article5. Nakamura T, Yabe Y. Histological anatomy of the triangular fibrocartilage complex of the human wrist. Ann Anat. 2000; 182:567–72.
Article6. Nakamura T, Sato K, Okazaki M, Toyama Y, Ikegami H. Repair of foveal detachment of the triangular fibrocartilage complex: open and arthroscopic transosseous techniques. Hand Clin. 2011; 27:281–90.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Technique for Repairing Foveal Tear of the Triangular Fibrocartilage Complex: Arthroscopic Knotless Repair
- Arthroscopic Repair of Triangular Fibrocartilage Complex Tear
- Open Repair of Triangular Fibrocartilage Complex Type 1B Tear
- Effective Functional Recovery after Triangular Fibrocartilage Complex Foveal Repair
- Arthroscopic Repair for Traumatic Peripheral Tear of Triangular Fibrocartilage Complex
