Early gastric cancer arising from heterotopic gastric mucosa in the gastric submucosa
- Affiliations
-
- 1Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. skim.kim@samsung.com
- 2Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2096641
- DOI: http://doi.org/10.4174/jkss.2011.80.Suppl1.S6
Abstract
- The incidence of heterotopic gastric mucosa located in the submucosa in resected stomach specimens has been reported to be 3.0 to 20.1%. Heterotopic gastric mucosa is thought to be a benign disease, which rarely becomes malignant. Heterotopic gastric mucosa exists in the gastric submucosa, and gastric cancer rarely occurs in heterotopic gastric mucosa. Since tumors are located in the normal submucosa, they appear as submucosal tumors during endoscopy, and are diagnosed through endoscopic biopsies with some difficulty. For such reasons, heterotopic gastric mucosa is mistaken as gastric submucosal tumor. Recently, two cases of early gastric cancer arising from heterotopic gastric mucosa in the gastric submucosa were treated. Both cases were diagnosed as submucosal tumors based on upper gastrointestinal endoscopy, endoscopic ultrasound, and computed tomography findings, and in both cases, laparoscopic wedge resections were performed, the surgical findings of which also suggested submucosal tumors. However, pathologic assessment of the surgical specimens led to the diagnosis of well-differentiated intramucosal adenocarcinoma arising from heterotopic gastric mucosa in the gastric submucosa.
MeSH Terms
Figure
-
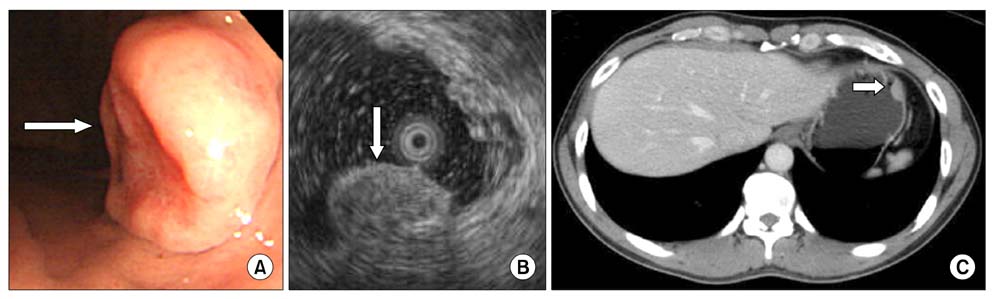
Fig. 1 (A) The endoscopic study revealed a 1.5 cm ovoid, elevated lesion with a central hyperemic depression on the anterior side of the high body. It was covered with normal-appearing mucosa, except for the central portion. (B) The endoscopic ultrasonographic study revealed a submucosal tumor that was 15.8 × 7.8 mm in size as a heterogenous hyperechoic lesion. (C) Abdominal computed tomography finding showed a 1.7 cm submucosal tumor in the gastric fundus.
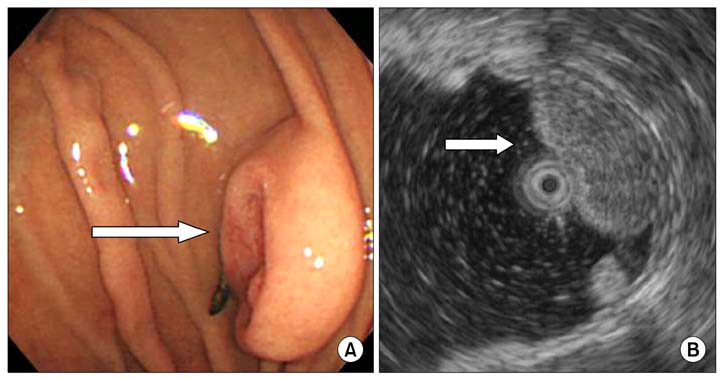
Fig. 2 (A) Follow-up endoscopic findings 6 months later revealed a submucosal tumor that was slightly increased in size. (B) Endoscopic ultrasonographic finding showed slightly increased size (about 18.8 mm).
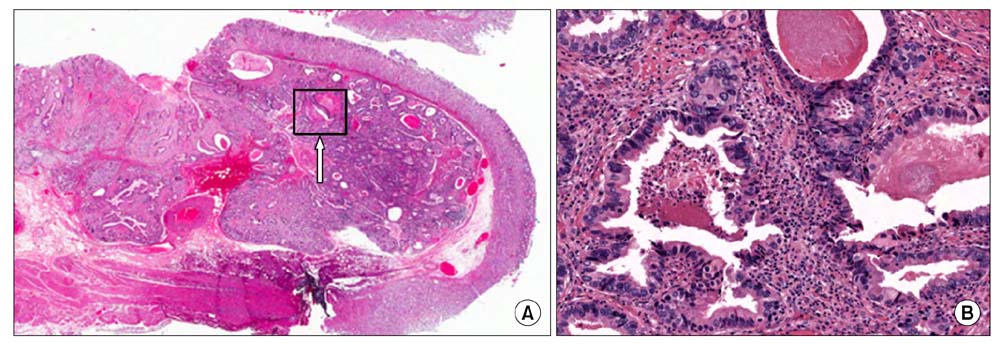
Fig. 3 (A) Low power view shows a 0.5 × 0.5 × 0.4 cm well-differentiated intramucosaladenocarcinoma arising from the heterotopic gastric mucosa in the gastric submucosa (H&E, ×40). (B) High power view shows a well-differentiated intramucosaladenocarioma (white arrow, H&E, ×400)
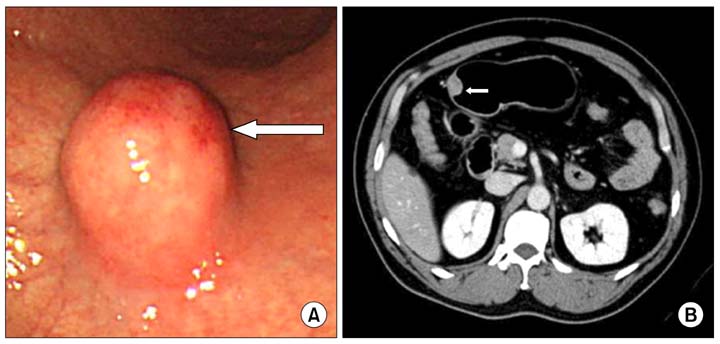
Fig. 4 (A) The endoscopic finding shows the submucosal tumor with normal mucosa on the greater curvature side of the proximal antrum, about 2 cm in size. A round, elevated lesion with normal covering mucosa, hard consistency, and central hyperemia was noted. (B) Abdominal computed tomography finding shows a 2 cm mass in the anterior wall of the gastric antrum.
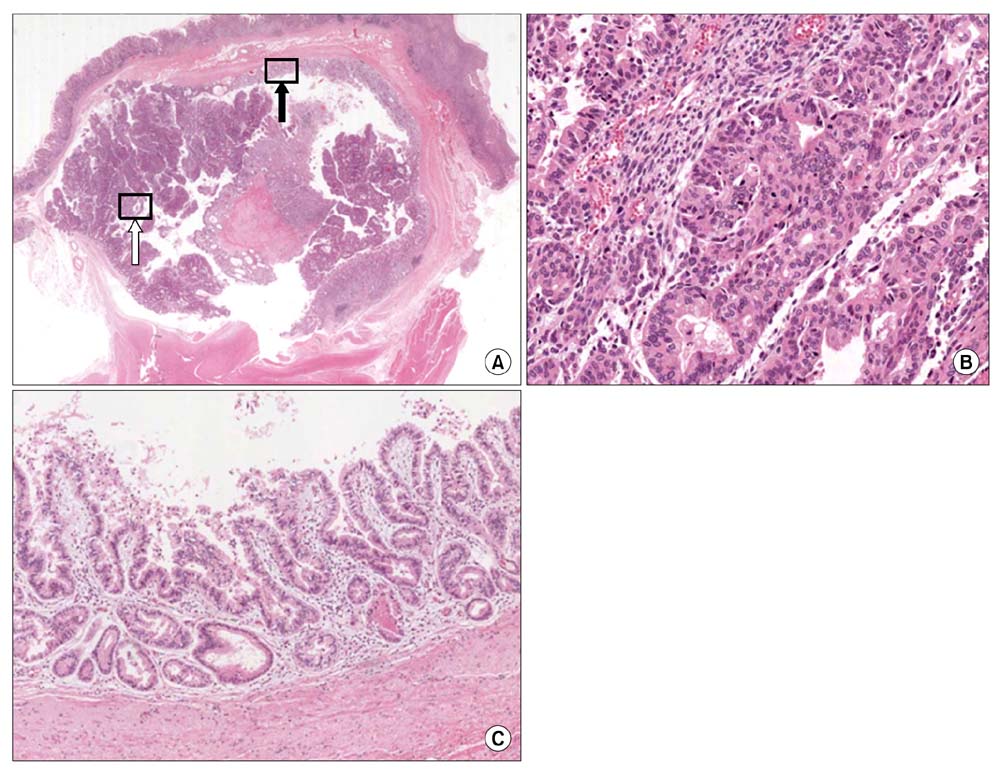
Fig. 5 (A) Low power view shows a 1.5 × 1.5 × 1 cm well-differentiated adenocarcinoma that did not invade the muscularis mucosa arising from the heterotopic gastric mucosa in the gastric submucosa (H&E, ×40). (B) High power view shows a well-differentiated adenocarcinoma (white arrow, H&E, ×400). (C) High power view shows heterotopic gastric mucosa in the gastric submucosa (black arrow, H&E, ×400).
Reference
-
1. Matsumoto K, Shida S, Murakami T, Sugiyama Y, Yamagata N, Tsuchida H, et al. Multiple submucosal cysts of the stomach associated with IIc + III type early gastric cancer: report of a case. Gan No Rinsho. 1987. 33:848–853.2. Yamagiwa H, Matsuzaki O, Ishihara A, Yoshimura H. Heterotopic gastric glands in the submucosa of the stomach. Acta Pathol Jpn. 1979. 29:347–350.3. Kosugi S, Kanda T, Hatakeyama K. Adenocarcinoma arising from heterotopic gastric mucosa in the stomach. J Gastroenterol Hepatol. 2006. 21:483–484.4. Rubio CA, Mandai K. Gastric adenocarcinomas in displaced mucosal glands. Anticancer Res. 1999. 19(3B):2381–2385.5. Tsujitani S, Oka S, Saito H, Kondo A, Ikeguchi M, Maeta M, et al. Less invasive surgery for early gastric cancer based on the low probability of lymph node metastasis. Surgery. 1999. 125:148–154.6. Otani Y, Ohgami M, Igarashi N, Kimata M, Kubota T, Kumai K, et al. Laparoscopic wedge resection of gastric submucosal tumors. Surg Laparosc Endosc Percutan Tech. 2000. 10:19–23.7. Iwanaga T, Koyama H, Takahashi Y, Taniguchi H, Wada A. Diffuse submucosal cysts and carcinoma of the stomach. Cancer. 1975. 36:606–614.8. Littler ER, Gleibermann E. Gastritis cystica polyposa. (Gastric mucosal prolapse at gastroenterostomy site, with cystic and infiltrative epithelial hyperplasia). Cancer. 1972. 29:205–209.9. Rubio CA. Intramucosal gastric cysts simulating submucosal cysts. Pathol Res Pract. 1989. 184:418–421.10. Tomonori A, Toshihiro S, Akimichi I, Sei K, Takeshi H, Hitoshi N, et al. Gastric cancer arising from ectopic gastric mucosa glands, report of a case. Stomach Intestine. 2003. 38:1551–1556.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Colonic Adenocarcinoma Arising from Gastric Heterotopia: A Case Study
- Heterotopic Gastric Mucosa in the Umbilicus
- Subepithelial Tumor-like Gastric Cancer
- A Case of the Endoscopic Removal of a Duodenal Heterotopic Gastric Mucosa Presenting as a Polypoid Lesion
- Two Cases of Huge Polypoid Early Gastric Cancer
