Incarcerated Obturator Hernia: The Need of Herniorrhaphy in Self-reduced Obturator Hernia
- Affiliations
-
- 1Department of Surgery, Chonnam National University Medical School, Gwangju, Korea. sgkim@jnu.ac.kr
- KMID: 2096543
- DOI: http://doi.org/10.4174/jkss.2009.76.3.192
Abstract
- An obturator hernia is an exceptionally rare form of hernia. It occurs mostly in elderly, thin, multiparous, and emaciated women. Correct diagnosis and treatment is important because delayed treatment can lead to a higher mortality rate. Recently, we experienced two cases of mechanical small bowel obstruction due to incarcerated obturator hernia. One of these patients was an 83-year-old woman who was diagnosed with left incarcerated obturator hernia by computed tomography (CT). The patient's symptom disappeared abruptly. A recheck CT scan revealed self-reduction of the obturator hernia, and the patient refused operation. Two weeks later, the patient was presented again to the emergency clinic with incarcerated small bowel in the left obturator hernia, which was seen on CT. The other patient was a 79-year-old woman who had a 2-day history of abdominal pain. She was diagnosed with a right obturator hernia by CT. Both patients were treated without bowel resection.
Keyword
MeSH Terms
Figure
-
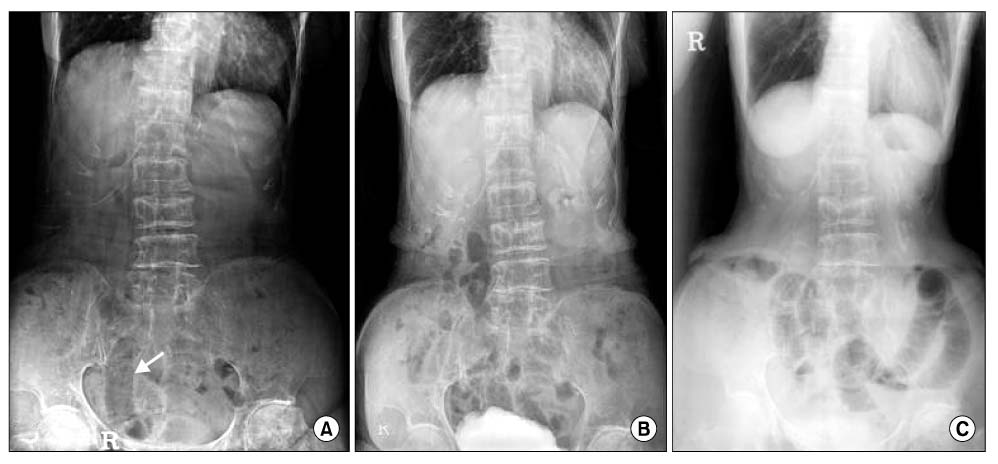
Fig. 1 Abdominal and pelvic radiographs of Case 1 in time series. (A) Local film shows a distended small bowel loop in the right side of the pelvis (arrow). (B) Normal bowel gas pattern is seen. (C) There are multiple gas-filled dilated small bowel loops. There is no colonic gas.

Fig. 2 Abdominal and pelvic CT scans of Case 1 in time series. (A) A small bowel segment is herniated through the left obturator foramen between pectineus and obturator externus muscle (arrow). (B) The left obturator canal is empty and dilated (arrow). (C) There is reherniated small bowel segment in the left obturator foramen (arrow).
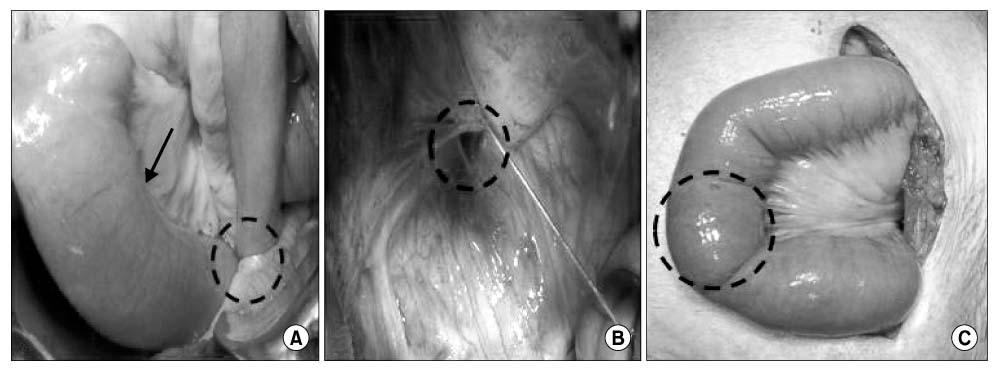
Fig. 3 Operative finding of Case 1. (A) The distal small bowel is herniated in the left obturator foramen (dotted circle), and the proximal portion of the small bowel is moderately distended (arrow). (B) The left obturator canal is seen. There is also a fibrous band between the upper margin of the left obturator foramen and the distal small bowel. (C) The viability of the small bowel segment which was herniated in the left obturator foramen seems good (dotted circle).

Fig. 4 Abdominal and pelvic radiograph of Case 2. Multiple gas-filled dilated small bowel loops without colonic gas suggest complete small bowel obstruction. The right lung field is severely collapsed by a fibrotic old tuberculous lesion. There is also a right-sided thoracic scoliosis.
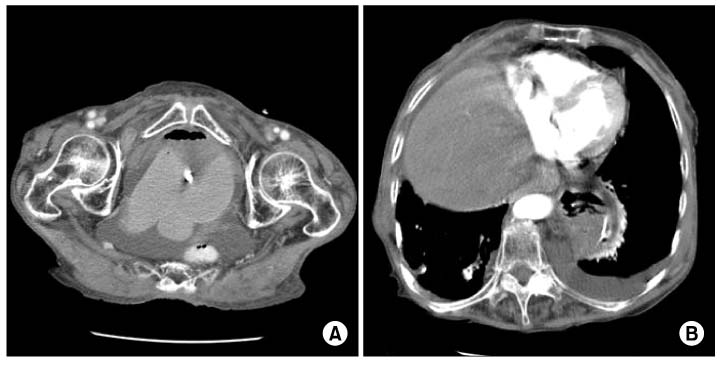
Fig. 5 Abdominal and pelvic CT scan of Case 2. (A) There is ascetic fluid collection in the pelvic cavity and a right-sided obturator hernia containing small bowel segment (arrow). (B) A coincidental left-sided paraesophageal hernia of the fundus of the stomach is seen.
Reference
-
1. Thanapaisan C, Thanapaisal C. Sixty-one cases of obturator hernia in Chiangrai Regional Hospital: retrospective study. J Med Assoc Thai. 2006. 89:2081–2085.2. Borchert D, Kumar B, Dennis R, Alberts J. Mesh migration following obturator hernia repair presenting as a bezoar inducing small intestinal obstruction. Hernia. 2008. 12:83–85.3. Bjork KJ, Mucha P Jr, Cahill DR. Obturator hernia. Surg Gynecol Obstet. 1988. 167:217–222.4. Sorabella RA, Miniati DN, Brandt ML. Laparoscopic obturator hernia repair in an adolescent. J Pediatr Surg. 2005. 40:e39–e41.5. Minkowski D, Komarowski G, Karon J. Atypical clinical picture of strangulated obturator hernia. Wiad Lek. 2006. 59:128–130.6. Kim YH, Lim DH, Kim BS, Hwang YH, Jeong YH. Small bowel obstruction due to incarcerated obturator hernia. J Korean Surg Soc. 2006. 71:73–78.7. Kammori M, Mafune K, Hirashima T, Kawahara M, Hashimoto M, Ogawa T, et al. Forty-three cases of obturator hernia. Am J Surg. 2004. 187:549–552.8. Yokoyama Y, Yamaguchi A, Isogai M, Hori A, Kaneoka Y. Thirty-six cases of obturator hernia: does computed tomography contribute to postoperative outcome? World J Surg. 1999. 23:214–216.9. Haraguchi M, Matsuo S, Kanetaka K, Tokai H, Azuma T, Yamaguchi S, et al. Obturator hernia in an ageing society. Ann Acad Med Singapore. 2007. 36:413–415.10. Shipkov CD, Uchikov AP, Grigoriadis E. The obturator hernia: difficult to diagnose, easy to repair. Hernia. 2004. 8:155–157.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Contralateral Obturator Hernia Immediately after a Right Obturator Herniorrhaphy: A Case Report
- Strangulated Obturator Hernia
- Totally Extraperitoneal Laparoscopic Repair of Obturator Hernia withPartial Intestinal Obstruction
- Obturator Hernia Which was Combined with Inguinal Hernia and Hiatal Hernia
- Strangulated obturator hernia
