J Rheum Dis.
2014 Apr;21(2):91-95. 10.4078/jrd.2014.21.2.91.
A Case of Persistent Apical Ballooning in a Patient with SLE
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Maryknoll Medical Center, Busan, Korea. ete@lycos.co.kr
- KMID: 2094664
- DOI: http://doi.org/10.4078/jrd.2014.21.2.91
Abstract
- Apical ballooning syndrome (ABS), also referred to as stress cardiomyopathy, is characterized by acute left ventricular dysfunction following a stressful situation. Diagnosis of ABS is made in the following scenarios: transient hypokinesia or dyskinesia of the left ventricular segment, absence of obstructive coronary disease, new electrocardiogram abnormalities, absence of recent significant head trauma, pheochromocytoma, myocarditis, and hypertrophic cardiomyopathy. Prognosis is usually favorable since the wall motion abnormality returns to normal within days, and certainly within the first month. We encountered a case of SLE with apical ballooning on echocardiography in a 44-year-old woman. She was suffering from severe left ventricular dysfunction that has persisted on 5 year follow-up echocardiography. We report this case along with a review of the relevant literature.
MeSH Terms
Figure
-
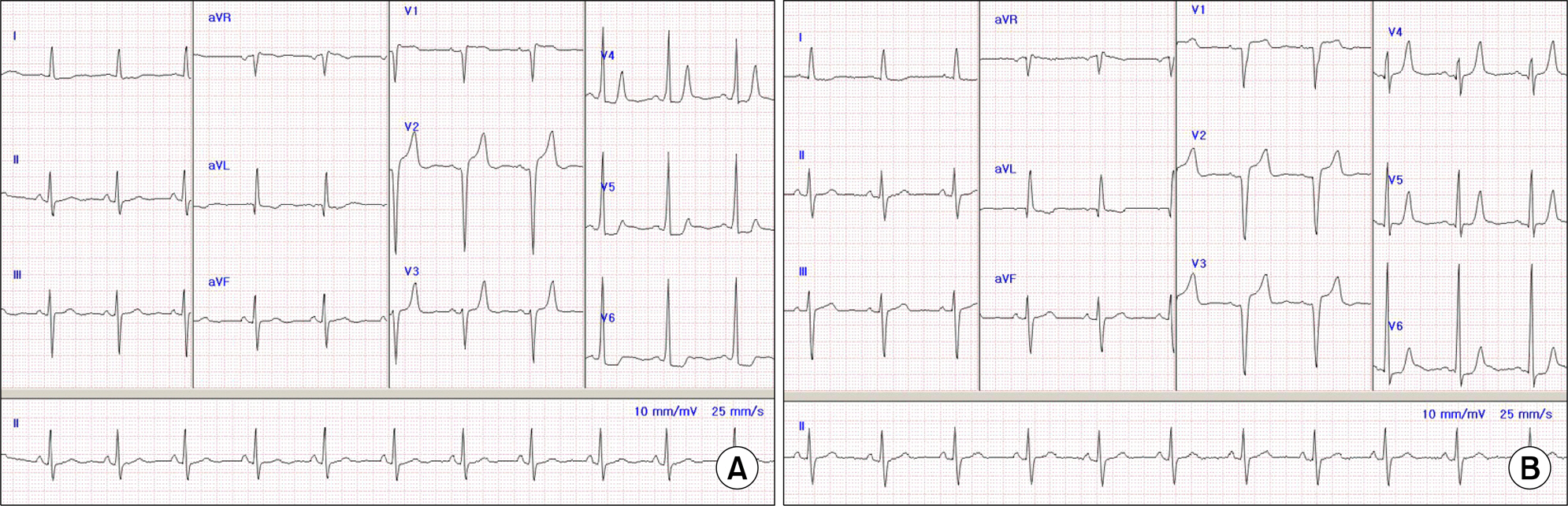
Figure 1. Electrocardiogram showing persistent ST-segment elevation during the first admission (A) and 5-year Follow-up (B).

Figure 2. Transthoracic echocardiography during the diastole (A), systole at first admission (B), during the diastole (C), systole (D) after 3-year Follow-up, during the diastole (E), systole (F) after 5-year Follow-up. It shows basal akinesia at mid to inferior wall with persistent apical ballooning.
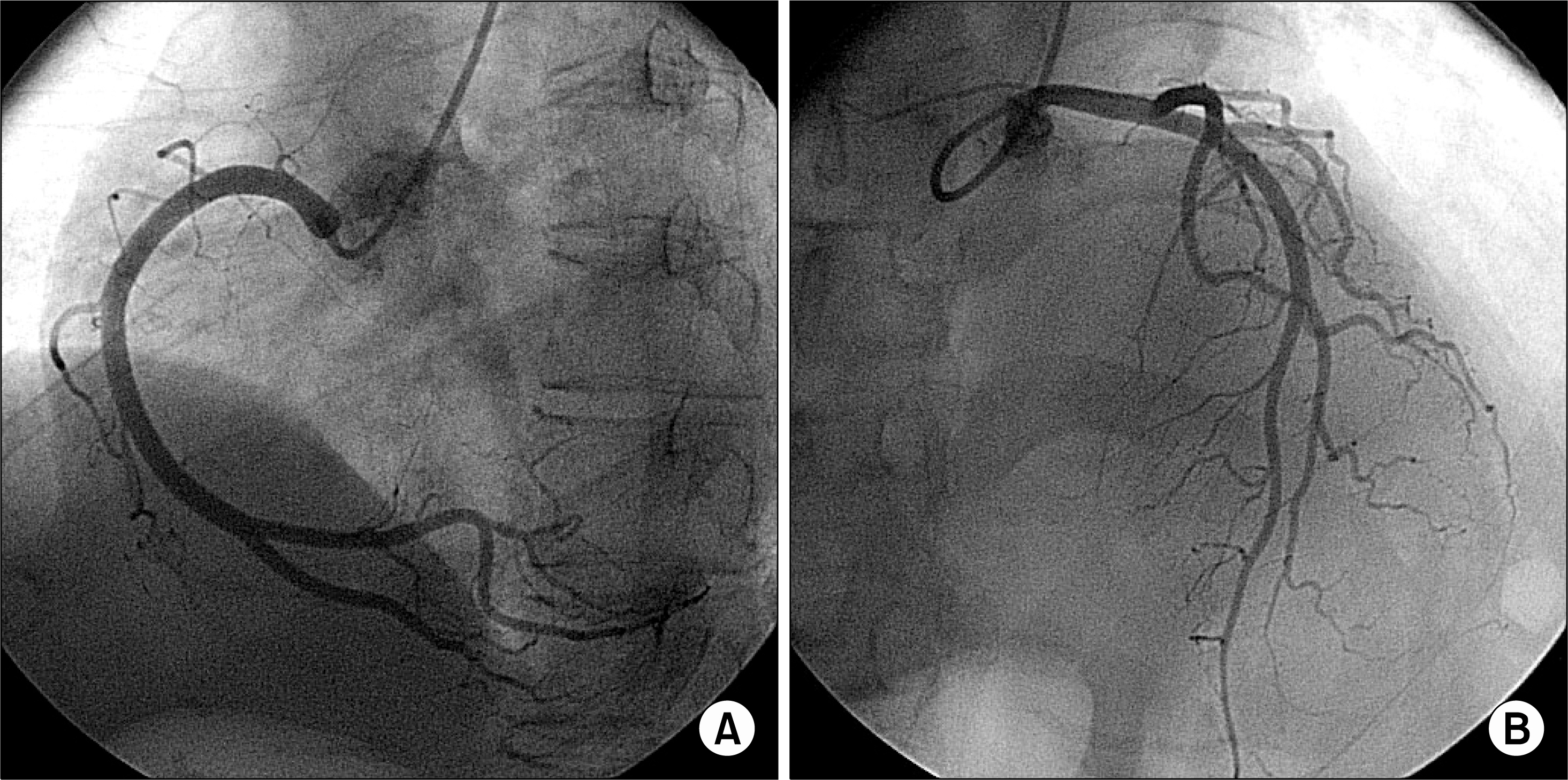
Figure 3. Coronary angiogram showed normal right (A) and left (B) coronary arteries.
Reference
-
1. Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. Am Heart J. 2008; 155:408–17.
Article2. Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006; 27:1523–9.
Article3. Zawadowski GM, Klarich KW, Moder KG, Edwards WD, Cooper LT Jr. A contemporary case series of lupus myocarditis. Lupus. 2012; 21:1378–84.
Article4. Appenzeller S, Pineau CA, Clarke AE. Acute lupus myocarditis: Clinical features and outcome. Lupus. 2011; 20:981–8.
Article5. Lim BA. Tako Tsubo cardiomyopathy in a patient with antiphosholipid syndrome secondary to systemic lupus er-ythemathosus (SLE). Med J Malaysia. 2008; 63:146–7.6. Matsuoka K, Okubo S, Fujii E, Uchida F, Kasai A, Aoki T, et al. Evaluation of the arrhythmogenecity of stress-induced “Takotsubo cardiomyopathy” from the time course of the 12-lead surface electrocardiogram. Am J Cardiol. 2003; 92:230–3.
Article7. Prasad A. Apical ballooning syndrome: An important differential diagnosis of acute myocardial infarction. Circulation. 2007; 115:e56–9.8. Wittstein IS, Thiemann DR, Lima JA, Baughman KL, Schulman SP, Gerstenblith G, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med. 2005; 352:539–48.
Article9. Amariles P. A comprehensive literature search: drugs as possible triggers of Takotsubo cardiomyopathy. Curr Clin Pharmacol. 2011; 6:1–11.
Article10. Yun MH, Choi S, Park JY, Kim CH, Beom JW, Park G, et al. Coincident Takotsubo Cardiomyopathy and Coronary Artery Disease. Korean J Med. 2012; 83:791–5.
Article11. Feldman AM, McNamara D. Myocarditis. N Engl J Med. 2000; 343:1388–98.
Article12. Barcin C, Kursaklioglu H, Kose S, Amasyali B, Isik E. Takotsubo cardiomyopathy in a patient with Addison disease: is apical ballooning always reversible? Int J Cardiol. 2010; 138:e15–7.
Article13. Ueda H, Hosokawa Y, Tsujii U, Miyawaki M, Mitsusada N, Yasuga Y, et al. An autopsy case of left ventricular apical ballooning probably caused by pheochromocytoma with persistent ST-segment elevation. Int J Cardiol. 2011; 149:e50–2.
Article14. Giugliano GR, Giugliano RP, Gibson CM, Kuntz RE. Meta-analysis of corticosteroid treatment in acute myocardial infarction. Am J Cardiol. 2003; 91:1055–9.
Article15. Eitel I, Lücke C, Grothoff M, Sareban M, Schuler G, Thiele H, et al. Inflammation in takotsubo cardiomyopathy: insights from cardiovascular magnetic resonance imaging. Eur Radiol. 2010; 20:422–31.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Persistent Apical Ballooning Complicated by Apical Thrombus in Takotsubo Cardiomyopathy of Systemic Lupus Erythematosus Patient
- Takotsubo Cardiomyopathy: A Case of Persistent Apical Ballooning Complicated by an Apical Mural Thrombus
- A case of transient mid-ventricular ballooning syndrome
- Biventricular Takotsubo Cardiomyopathy Associated with Epilepsy
- Magnetic Resonance Imaging of Transient Left Ventricular Apical Ballooning Related to Emotional Stress: a Case Report
