Early Detection of Perforation of the Right Ventricle by a Permanent Pacemaker Lead
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Sanggye Paik Hospital, Inje University Medical College, Seoul, Korea. cardiobk@sanggyepaik.ac.kr
- KMID: 2093984
- DOI: http://doi.org/10.4070/kcj.2007.37.9.453
Abstract
- Ventricular perforation is a rare complication of permanent cardiac pacemaker implantation. We report here on a 68-year-old woman with a dual chamber permanent pacemaker that had been implanted one month earlier, and she suffered cardiac perforation from the pacemaker lead. Frequent follow-up via12-lead surface electrocardiography and chest radiography and the proper work-up for pacemaker implantation are needed for detecting rare complications after pacemaker implantation.
Keyword
Figure
-
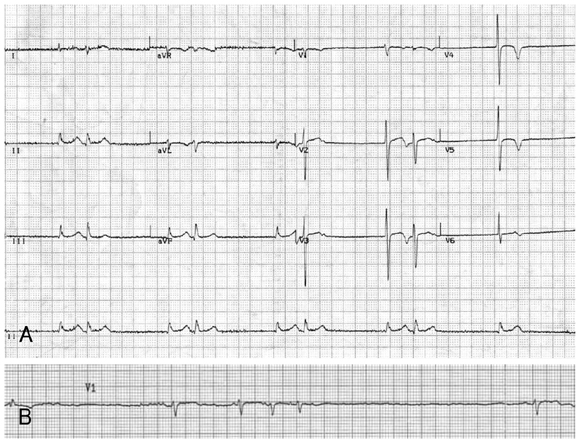
Fig. 1 The initial electrocardiograph (ECG) revealed junctional rhythm without a sinus p wave (A) and the longest pause was 3.45 sec (B).

Fig. 2 The chest posteroanterior and lateral films showed no significant interval change of the dual-chamber pacemaker electrodes, with the tip of each lead positioned in the right atrium and right ventricle, between two days after the procedure (A, B) and post-procedure day 32 (C, D). PA: posteroanterior, Lt: left.
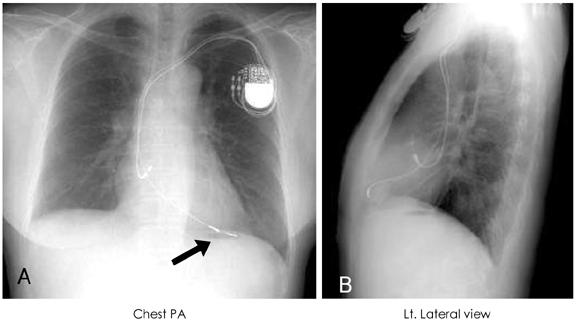
Fig. 3 36 days after pacemaker implantation, the chest radiographs show the antero-inferiorly displaced ventricular lead (arrow) beyond the cardiac shadow (A, B). PA: posteroanterior, Lt: left.
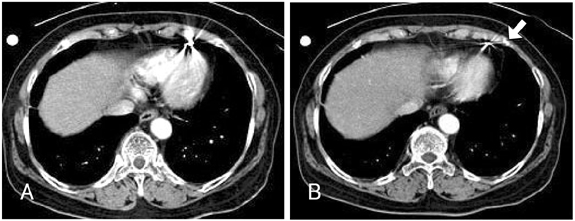
Fig. 4 Axial scan of chest computed tomography demonstrated that the tip of the pacemaker lead (arrow) was located in the pericardial fat layer near the pericardium at 36 days after procedure (A, B).
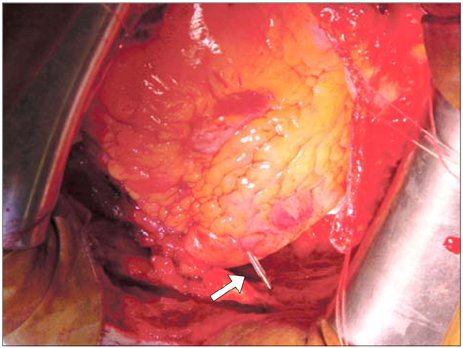
Fig. 5 The thoracotomy view showing the exposed pericardial sac. The tip of the ventricular lead (arrow) protruded through the right ventricle apex without causing pericardial effusion or hematoma.

Fig. 6 The AV conduction was normal (Fig. 6. ECG). AV: atrioventricular, ECG: electrocardiograph.
Reference
-
1. Ellenbogen KA, Hellkamp AS, Wilkoff BL, et al. Complications arising after implantation of DDD pacemakers: the MOST experience. Am J Cardiol. 2003. 92:740–741.2. Choi JH, Rhim CY, Hong KS, et al. Four cases of pericardial tamponade following percutaneous transluminal coronary angioplasty. Korean Circ J. 1999. 29:523–527.3. Parsonnet V, Bernstein AD, Lindsay B. Pacemaker implantation complication rates: an analysis of some contributing factors. J Am Coll Cardiol. 1989. 13:917–921.4. Aykol A, Aydin A, Erdinler I, Oguz E. Late perforation of the heart, pericardium, and diaphragm by an active-fixation ventricular lead. Pacing Clin Electrophysiol. 2005. 28:350–351.5. Mahapatra S, Bybee KA, Bunch TJ, et al. Incidence and predictors of cardiac perforation after permanent pacemaker placement. Heart Rhythm. 2005. 2:907–911.6. Zehender M, Buchner C, Meinertz T, Just H. Prevalence, circumstances, mechanisms, and risk stratification of sudden cardiac death in unipolar single-chamber ventricular pacing. Circulation. 1992. 85:596–605.7. Garcia-Bolao I, Teijeira R, Diaz-Dorronsoro I. Late fatal right ventricular perforation as complication of permanent pacing leads. Pacing Clin Electrophysiol. 2001. 24:1036–1037.8. Sanoussi A, El Nakadi B, Lardinois B, De Bruyne Y, Joris M. Late right ventricular perforation after permanent pacemaker implantation: how far can the lead go. Pacing Clin Electrophysiol. 2005. 28:723–725.9. Henrikson CA, Leng CT, Yuh DD, Brinker JA. Computed tomography to assess possible cardiac lead perforation. Pacing Clin Electrophysiol. 2006. 29:509–511.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Right Ventricular Perforation and Left Hemothorax by Permanent Transveneous Pacemaker Lead: Report of 1 Case
- A Unique Case of Non-Capture of Permanent Pacemaker Lead: Delayed Lead Perforation and Cardiac Tamponade
- Infected Endocarditis Related Pacemaker leads: A Case Report
- Permanent Pacemaker Lead Induced Severe Tricuspid Regurgitation in Patient Undergoing Multiple Valve Surgery
- A Case of Pacemaker Implantation after Balloon Venoplasty on Innominate Vein Stenosis
