Tumor Lysis Syndrome in Lymphoblastic Crisis of CML
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Hanyang University, Seoul, Korea. kimis@hanyang.ac.kr
- KMID: 2083487
- DOI: http://doi.org/10.5045/kjh.2006.41.2.119
Abstract
- Tumor lysis syndrome (TLS) defines the metabolic derangements that occur with tumor breakdown following the initiation of cytotoxic therapy. TLS results from the rapid destruction of malignant cells and the abrupt release of intracellular materials and their metabolites into the extracellular space. The syndrome causes hyperuricemia, hyperkalemia, hyperphosphatemia, secondary hypocalcemia and uremia. It can result in acute renal failure and be fatal. Early recognition of patient at risk and preventive measures are important. There is a high incidence of TLS in tumors with high proliferative rates and large burden such as acute lymphoblastic leukemia and Burkitt's lymphoma. It less commonly occurs in solid tumors such as testicular cancer, breast cancer and small cell lung cancer. There are only a few reports on TLS complicated in CML in blast crisis. So we report a 45-yr-old woman presenting with TLS associated with CML in lymphoblastic crisis after the initiation of cytotoxic chemotherapy.
MeSH Terms
Figure
-
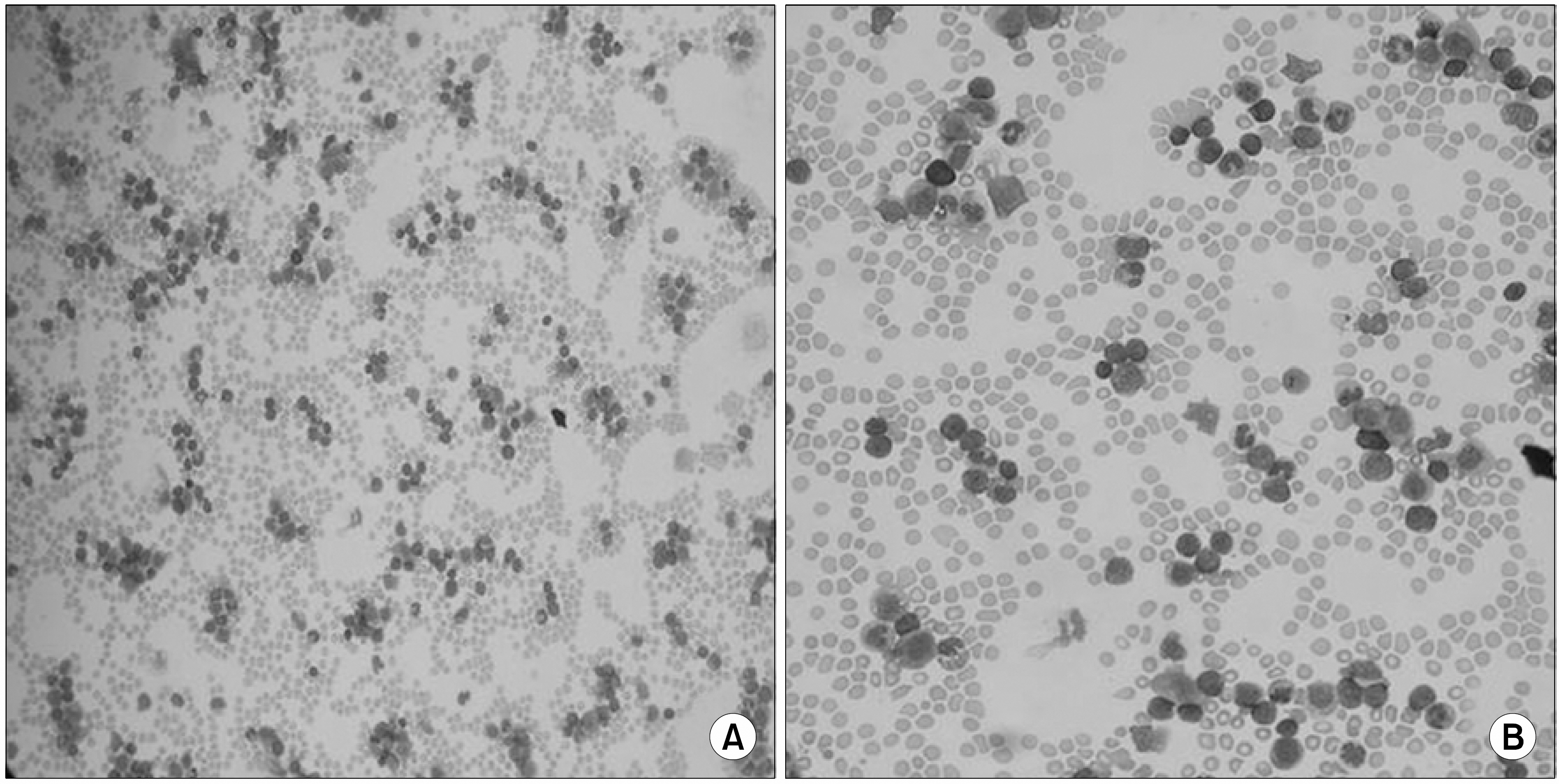
Fig. 1 Peripheral blood smear. Marked leukocytosis composed of immature blasts (44%), band form (5%), promyelocyte (3%), myelocyte (10%), metamyelocyte (7%), segmented neutrophils (13%), eosinophils (3%), monocyte (2%) and lymphocytes (9%) is observed. Moderate decrease of platelet component is also observed. (A) ×40, (B) ×200.
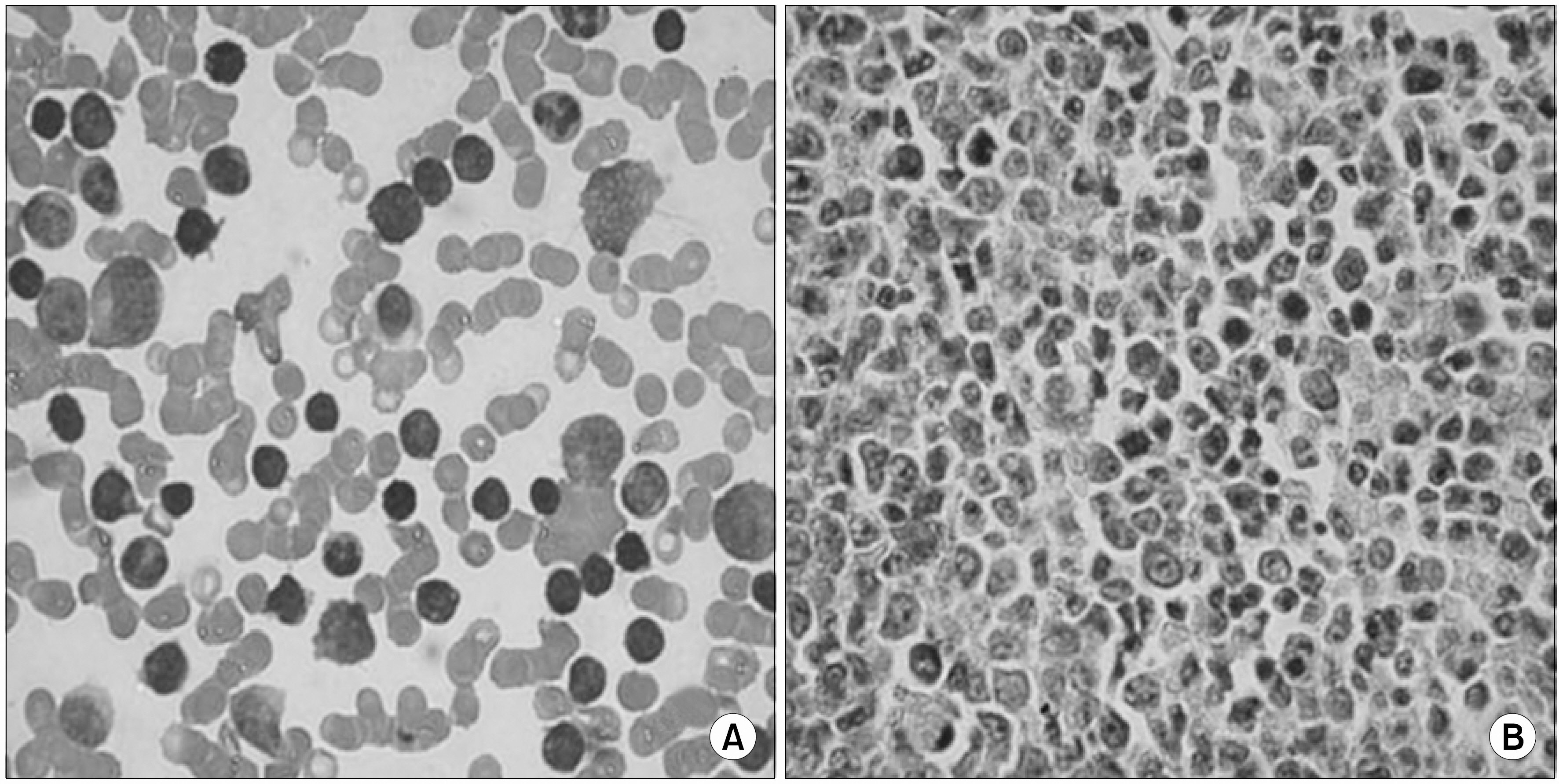
Fig. 2 Bone marrow biopsy. (A) Bone marrow biopsy imprint (touch preparation), More than 30% of all hematopoietic cells are replaced by immature cells. These cells show high nuclear/ cytoplasmic ratio, one or more prominent nucleoli, and fine nuclear chromatin. These cells also vary in size from medium to large. The myeloid series are increased in proportion and reveal normal maturation. The erythroid series are decreased in proportion and reveal normal maturation. The megakaryocytes are decreased in number. (B) The bone marrow section is hypercellular (90%) for her age. Immature cells are seen throughout section intermingled with other hematopoietic cells.
Reference
-
1). Davidson MB., Thakkar S., Hix JK., Bhandarkar ND., Wong A., Schreiber MJ. Pathophysiology, clinical consequences, and treatment of tumor lysis syndrome. Am J Med. 2004. 116:546–54.
Article2). Woo IS., Kim JS., Park MJ, et al. Spontaneous acute tumor lysis syndrome with advanced gastric cancer. J Korean Med Sci. 2001. 16:115–8.
Article3). Lee CC., Wu YH., Chung SH., Chen WJ. Acute tumor lysis syndrome after thalidomide therapy in advanced hepatocellular carcinoma. Oncologist. 2006. 11:87–8.
Article4). Baeksgaard L., Sorensen JB. Acute tumor lysis syndrome in solid tumors—a case report and review of the literature. Cancer Chemother Pharmacol. 2003. 51:187–92.
Article5). Wright JL., Lin DW., Dewan P., Montgomery RB. Tumor lysis syndrome in a patient with metastatic, androgen independent prostate cancer. Int J Urol. 2005. 12:1012–3.
Article6). Chen SW., Hwang WS., Tsao CJ., Liu HS., Huang GC. Hydroxyurea and splenic irradiation-induced tumour lysis syndrome: a case report and review of the literature. J Clin Pharm Ther. 2005. 30:623–5.
Article7). Spinazze S., Schrijvers D. Metabolic emergencies. Crit Rev Oncol Hematol. 2006. 58:79–89.
Article8). Cairo MS., Bishop M. Tumour lysis syndrome: new therapeutic strategies and classification. Br J Haematol. 2004. 127:3–11.
Article9). Annemans L., Moeremans K., Lamotte M, et al. Incidence, medical resource utilisation and costs of hyperuricemia and tumour lysis syndrome in patients with acute leukaemia and non-Hodgkin's lymphoma in four European countries. Leuk Lymphoma. 2003. 44:77–83.
Article10). Hussain K., Mazza JJ., Clouse LH. Tumor lysis syndrome (TLS) following fludarabine therapy for chronic lymphocytic leukemia (CLL): case report and review of the literature. Am J Hematol. 2003. 72:212–5.
Article11). Vora A., Bhutani M., Sharma A., Raina V. Severe tumor lysis syndrome during treatment with STI 571 in a patient with chronic myelogenous leukemia accelerated phase. Ann Oncol. 2002. 13:1833–4.12). Przepiorka D., Gonzales-Chambers R. Acute tumor lysis syngdrome in a patient with chronic myelogenous leukemia in blast crisis: role of high-dose Ara-C. Bone Marrow Transplant. 1990. 6:281–2.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Tumor Lysis Syndrome Presenting Acute Kidney Injury with Extreme Hyperuricemia and Urinary Stone: A Rare Case of Spontaneous Tumor Lysis Syndrome
- Two Cases of Chronic Myeloid Leukemia in Lymphoid Blast Phase Presented as Philadelphia-Positive Acute Lymphoblastic Leukemia
- A Case of T-cell Acute Lymphoblastic Leukemia presented with Spontaneous Tumor Lysis Syndrome and Superior Bena Cava Syndrome
- Extramedullary B Lymphoblastic Crisis of CML, Presenting as a Leptomeningeal Tumor: A Case Report
- ider (9) (q10)t (9;22) (q34;q11.2) as Secondary Karyotypic Aberration of Chronic Myelogeous Leukemia
