Correlation between Femoral Guidewire Position and Tunnel Communication in Double Bundle Anterior Cruciate Ligament Reconstruction
- Affiliations
-
- 1Department of Orthopaedic Surgery and Institute of Health Sciences, School of Medicine, Gyeongsang National University, Gyeongsang National University Hospital, Jinju, Korea. hscspine@hanmail.net
- 2Department of Thoracic and Cardiovascular Surgery and Institute of Health Sciences, School of Medicine, Gyeongsang National University, Gyeongsang National University Hospital, Jinju, Korea.
- KMID: 2070207
- DOI: http://doi.org/10.3349/ymj.2014.55.6.1592
Abstract
- PURPOSE
The object of this study was to determine the shortest possible distances of antero-medial (AM) and postero-lateral (PL) guide wire tunnel positions required to prevent femoral bone tunnel communication in double-bundle anterior cruciate ligament (ACL) reconstruction using human cadaver knees.
MATERIALS AND METHODS
The centers of femoral AM and PL bundles of 16 cadaveric knees were drilled with guide wires and the distances of guide wires, were measured upon entrance into the bone. Femoral tunnel drilling was performed using transportal technique. The diameters of AM and PL graft were 8 mm and 6 mm, respectively. CT scans were taken on each knee, and 3-dimensional models were constructed to identify the femoral tunnel position and to create AM and PL tunnel virtual cylinders. Thickness of the bone bridge between the two tunnels was measured.
RESULTS
In four out of six specimens, in which the guide wires were placed at less than or equal to 9 mm, communication was noted. In specimens with guide wires placed at distances greater than or equal to 10 mm, communication was not noted. The two groups showed a statistically significant difference (p=0.008). In cases where the distance between the AM and PL femoral tunnel guide wires was 12 mm, the bone bridge thickness was greater than 2 mm along the tunnel.
CONCLUSION
The technique for double bundle-anterior cruciate ligament (DB-ACL) reconstruction that we show here can avoid bone tunnel communication when AM and PL femoral guide wires are placed at least 10 mm apart, and 12 mm should be kept to preserve 2 mm bone bridge thickness.
MeSH Terms
Figure
-
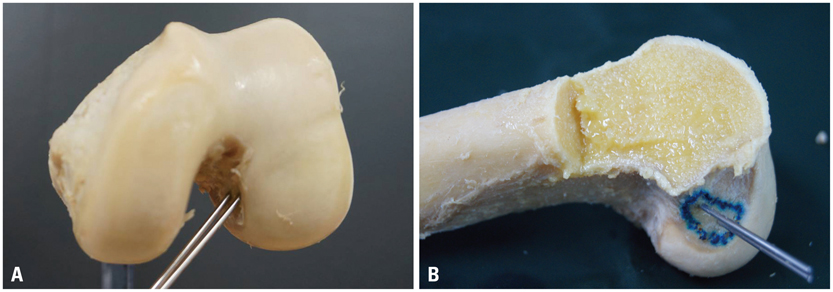
Fig. 1 Guide wires were inserted through the center of the femoral anteromedial and posterolateral footprint of the anterior cruciate ligament at angle of 45° in the axial plane on knees flexed at 110°. Two guide wires were inserted in cadaveric femur: (A) Anteroposterior view. (B) Lateral view.
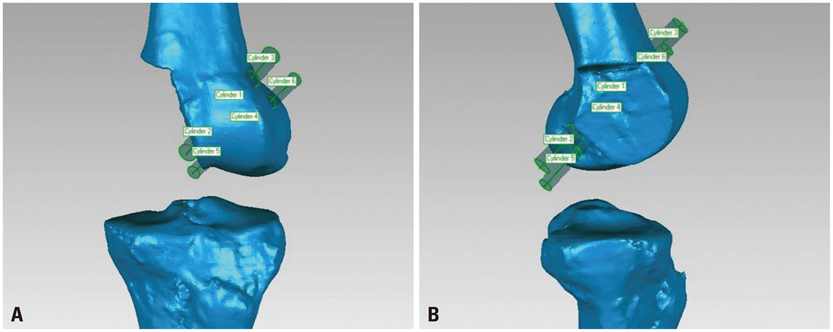
Fig. 2 The virtual anteromedial and posterolateral tunnel cylinders were created at the femoral side using Geomagic Software (Research Triangle Park, NC, USA) and bone bridge thickness were measured. (A) Anteroposterior view. (B) Lateral view.
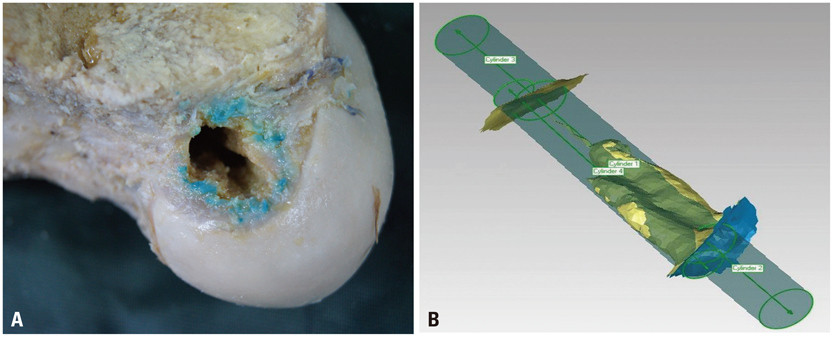
Fig. 3 Tunnel communication caused by drilling was observed. (A) At the level of the enterance by gross specimen. (B) Along the whole tunnel using a 3 dimensional virtual cylinder model.
Cited by 1 articles
-
A Comparison between Clinical Results of Selective Bundle and Double Bundle Anterior Cruciate Ligament Reconstruction
Yon-Sik Yoo, Si Young Song, Cheol Jung Yang, Jong Mun Ha, Yoon Sang Kim, Young-Jin Seo
Yonsei Med J. 2016;57(5):1199-1208. doi: 10.3349/ymj.2016.57.5.1199.
Reference
-
1. Gianotti SM, Marshall SW, Hume PA, Bunt L. Incidence of anterior cruciate ligament injury and other knee ligament injuries: a national population-based study. J Sci Med Sport. 2009; 12:622–627.
Article2. Muller B, Hofbauer M, Wongcharoenwatana J, Fu FH. Indications and contraindications for double-bundle ACL reconstruction. Int Orthop. 2013; 37:239–246.
Article3. Schreiber VM, van Eck CF, Fu FH. Anatomic Double-bundle ACL Reconstruction. Sports Med Arthrosc. 2010; 18:27–32.
Article4. Fu FH, Shen W, Starman JS, Okeke N, Irrgang JJ. Primary anatomic double-bundle anterior cruciate ligament reconstruction: a preliminary 2-year prospective study. Am J Sports Med. 2008; 36:1263–1274.
Article5. Mae T, Shino K, Miyama T, Shinjo H, Ochi T, Yoshikawa H, et al. Single-versus two-femoral socket anterior cruciate ligament reconstruction technique: biomechanical analysis using a robotic simulator. Arthroscopy. 2001; 17:708–716.
Article6. Muneta T, Koga H, Mochizuki T, Ju YJ, Hara K, Nimura A, et al. A prospective randomized study of 4-strand semitendinosus tendon anterior cruciate ligament reconstruction comparing single-bundle and double-bundle techniques. Arthroscopy. 2007; 23:618–628.
Article7. Yagi M, Wong EK, Kanamori A, Debski RE, Fu FH, Woo SL. Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med. 2002; 30:660–666.
Article8. Yasuda K, Kondo E, Ichiyama H, Tanabe Y, Tohyama H. Clinical evaluation of anatomic double-bundle anterior cruciate ligament reconstruction procedure using hamstring tendon grafts: comparisons among 3 different procedures. Arthroscopy. 2006; 22:240–251.
Article9. Neven E, D'Hooghe P, Bellemans J. Double-bundle anterior cruandciate ligament reconstruction: a cadaveric study on the posterolateral tunnel position and safety of the lateral structures. Arthroscopy. 2008; 24:436–440.
Article10. Tsukada H, Ishibashi Y, Tsuda E, Fukuda A, Toh S. Anatomical analysis of the anterior cruciate ligament femoral and tibial footprints. J Orthop Sci. 2008; 13:122–129.
Article11. Hantes ME, Liantsis AK, Basdekis GK, Karantanas AH, Christel P, Malizos KN. Evaluation of the bone bridge between the bone tunnels after anatomic double-bundle anterior cruciate ligament reconstruction: a multidetector computed tomography study. Am J Sports Med. 2010; 38:1618–1625.
Article12. Christel P, Sahasrabudhe A, Basdekis G. Anatomic double-bundle anterior cruciate ligament reconstruction with anatomic aimers. Arthroscopy. 2008; 24:1146–1151.
Article13. Pombo MW, Shen W, Fu FH. Anatomic double-bundle anterior cruciate ligament reconstruction: where are we today? Arthroscopy. 2008; 24:1168–1177.
Article14. Zantop T, Wellmann M, Fu FH, Petersen W. Tunnel positioning of anteromedial and posterolateral bundles in anatomic anterior cruciate ligament reconstruction: anatomic and radiographic findings. Am J Sports Med. 2008; 36:65–72.
Article15. Petersen W, Tretow H, Weimann A, Herbort M, Fu FH, Raschke M, et al. Biomechanical evaluation of two techniques for double-bundle anterior cruciate ligament reconstruction: one tibial tunnel versus two tibial tunnels. Am J Sports Med. 2007; 35:228–234.
Article16. Steckel H, Starman JS, Baums MH, Klinger HM, Schultz W, Fu FH. The double-bundle technique for anterior cruciate ligament reconstruction: a systematic overview. Scand J Med Sci Sports. 2007; 17:99–108.
Article17. Lind M, Feller J, Webster KE. Bone tunnel widening after anterior cruciate ligament reconstruction using EndoButton or EndoButton continuous loop. Arthroscopy. 2009; 25:1275–1280.
Article18. Wilson TC, Kantaras A, Atay A, Johnson DL. Tunnel enlargement after anterior cruciate ligament surgery. Am J Sports Med. 2004; 32:543–549.
Article19. Basdekis G, Abisafi C, Christel P. Effect of knee flexion angle on length and orientation of posterolateral femoral tunnel drilled through anteromedial portal during anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2009; 25:1108–1114.
Article20. Lehmann AK, Osada N, Zantop T, Raschke MJ, Petersen W. Femoral bridge stability in double-bundle ACL reconstruction:impact of bridge width and different fixation techniques on the structural properties of the graft/femur complex. Arch Orthop Trauma Surg. 2009; 129:1127–1132.
Article21. Chae IJ, Bae JH, Wang JH, Jeon J, Park JH. Double-bundle anterior cruciate ligament reconstruction with split Achilles allograft and single tibia tunnel for small ACL tibial footprint: technical note with clinical results. Arch Orthop Trauma Surg. 2013; 133:819–825.
Article22. Tajima T, Chosa E, Yamamoto K, Yamaguchi N. Arthroscopic anatomical double-bundle anterior cruciate ligament reconstruction for asian patient using a bone-patellar tendon-bone and gracilis tendon composite autograft: a technical note. Sports Med Arthrosc Rehabil Ther Technol. 2012; 4:9.
Article23. Bernard M, Hertel P, Hornung H, Cierpinski T. Femoral insertion of the ACL. Radiographic quadrant method. Am J Knee Surg. 1997; 10:14–21.24. Hensler D, Working ZM, Illingworth KD, Thorhauer ED, Tashman S, Fu FH. Medial portal drilling: effects on the femoral tunnel aperture morphology during anterior cruciate ligament reconstruction. J Bone Joint Surg Am. 2011; 93:2063–2071.
Article25. Lee YS, Lee SW, Nam SW, Oh WS, Sim JA, Kwak JH, et al. Analysis of tunnel widening after double-bundle ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2012; 20:2243–2250.
Article26. Clatworthy MG, Annear P, Bulow JU, Bartlett RJ. Tunnel widening in anterior cruciate ligament reconstruction: a prospective evaluation of hamstring and patella tendon grafts. Knee Surg Sports Traumatol Arthrosc. 1999; 7:138–145.
Article27. Ahn JH, Park JS, Lee YS, Cho YJ. Femoral bioabsorbable cross-pin fixation in anterior cruciate ligament reconstruction. Arthroscopy. 2007; 23:1093–1099.
Article28. L'Insalata JC, Klatt B, Fu FH, Harner CD. Tunnel expansion following anterior cruciate ligament reconstruction: a comparison of hamstring and patellar tendon autografts. Knee Surg Sports Traumatol Arthrosc. 1997; 5:234–238.29. Siebold R, Cafaltzis K. Differentiation between intraoperative and postoperative bone tunnel widening and communication in double-bundle anterior cruciate ligament reconstruction: a prospective study. Arthroscopy. 2010; 26:1066–1073.
Article30. Järvelä T, Moisala AS, Paakkala T, Paakkala A. Tunnel enlargement after double-bundle anterior cruciate ligament reconstruction: a prospective, randomized study. Arthroscopy. 2008; 24:1349–1357.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Single Bundle Anterior Cruciate Ligament Reconstruction
- The Correlation of Tunnel Position, Orientation and Tunnel Enlargement in Outside-in Single-Bundle Anterior Cruciate Ligament Reconstruction
- Double-Bundle Anterior Cruciate Ligament Reconstruction
- Femoral Tunnel Drilling Techniques in Anterior Cruciate Ligament Reconstruction
- Anatomic Single Bundle Anterior Cruciate Ligament Reconstruction by Low Accessory Anteromedial Portal Technique: An In Vivo 3D CT Study
