Ligament Preserving Technique for a Locked Metacarpophalangeal Joint of the Index Finger
- Affiliations
-
- 1Department of Orthopedic Surgery, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea. kbsos@schmc.ac.kr
- KMID: 2069882
- DOI: http://doi.org/10.4055/cios.2015.7.1.104
Abstract
- BACKGROUND
Locking of metacarpophalangeal joint (MPJ) of the index finger occurs when volar radial osteophytes of the metacarpal head catch the accessory collateral ligament. We devised a ligament-preserving approach to quickly restore the MPJ motion while protecting the radial collateral ligament.
METHODS
We retrospectively reviewed the results of nine patients treated for a locked MPJ of the index finger. In three patients, closed reduction was successful. In six cases, volar radial osteophytes were excised from the metacarpal head using a ligament-preserving technique through a longitudinal incision on the radial side. We analyzed osteophyte shape and height as demonstrated by X-ray and computed tomography (CT). Function was evaluated by examining the range of motion, recurrence, Disabilities of the Arm, Shoulder and Hand (DASH) score, and MPJ stability based on the key pinch strength. One male and eight female patients were followed for an average of 33 months (range, 12 to 65 months); the average age of patients was 41 years (range, 34 to 47 years). The average duration of locking of the MPJ was 23 days (range, 1 to 53 days).
RESULTS
The sharp type of osteophytes was identified in six patients and the blunt type of osteophytes was indentified in three patients. The average height of radial osteophytes on the index finger metacarpal was 4.6 +/- 0.4 mm in the axial CT image. At the final follow-up, the average extension limitation decreased from 26degrees (range, 10degrees to 45degrees) to 0degrees, and further flexion increased from 83degrees (range, 80degrees to 90degrees) to 86degrees. There was no recurrent locking after surgery. The DASH score improved from 24.3 to 7.2. Key pinch strength improved from 67.3% to 90.4%.
CONCLUSIONS
We obtained satisfactory outcomes in irreducible locking of the MPJ of the index finger by excising volar radial osteophytes of the metacarpal head using a ligament-preserving approach.
Keyword
MeSH Terms
Figure
-

Fig. 1 Radiographs of the metacarpal head. (A) A sharp edge (case 4). (B) A blunt edge (case 9).
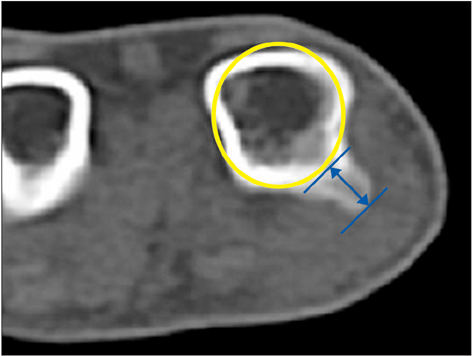
Fig. 2 Height of metacarpal head osteophytes of the index finger. The osteophyte height is defined as the distance between the base of the condyle and the most prominent radial margin of the osteophyte (arrow). Metacarpal diameter is measured from a circle template. Template of metacarpal head (yellow circle).
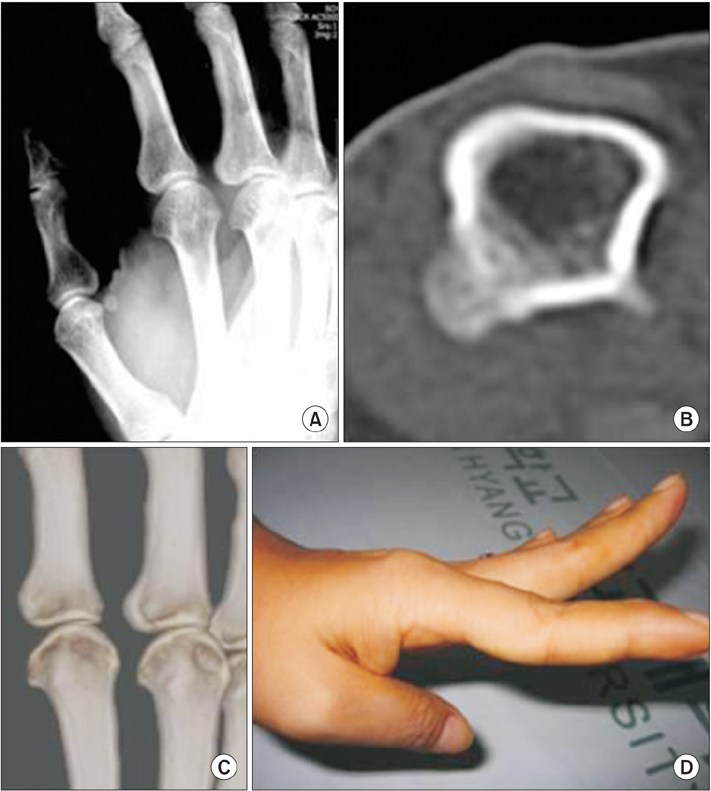
Fig. 3 A 46-year-old female patient (case 6) with a locked metacarpophalangeal joint (MPJ) of the index finger. (A) Oblique radiograph shows a sharp edge of the index metacarpal radial condyle. Axial (B) and three-dimensional (C) computed tomography images show radial osteophyte of the index metacarpal head. (D) Index MPJ extension was limited prior to surgery.
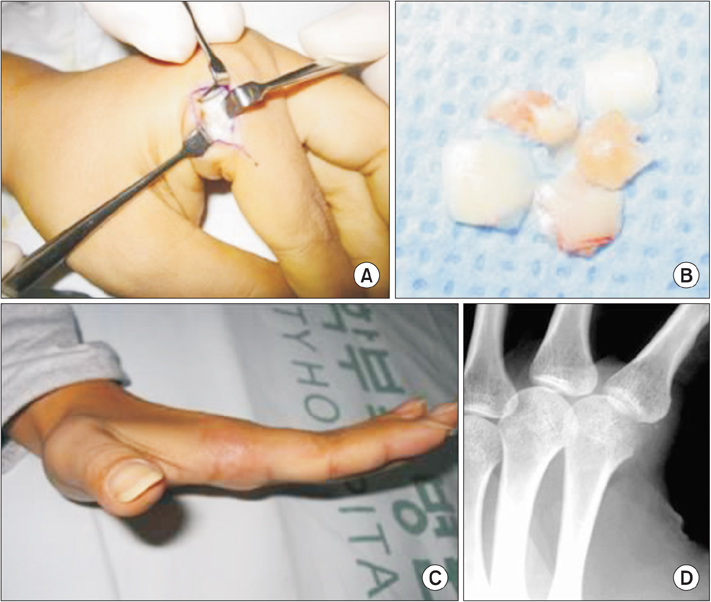
Fig. 4 A 34-year-old female patient (case 2) with a locked metacarpophalangeal joint (MPJ) of the index finger. (A) Intraoperative photograph during ligament-preserving surgery on the flexed index MPJ with a radial osteophyte on the metacarpal head. (B) Osteophyte fragment was removed from the radial metacarpal head using a mini-osteotome. (C) Postoperative photograph shows full extension of the MPJ. (D) Postoperative oblique radiograph does not show a visible sharp edge of the index metacarpal head.
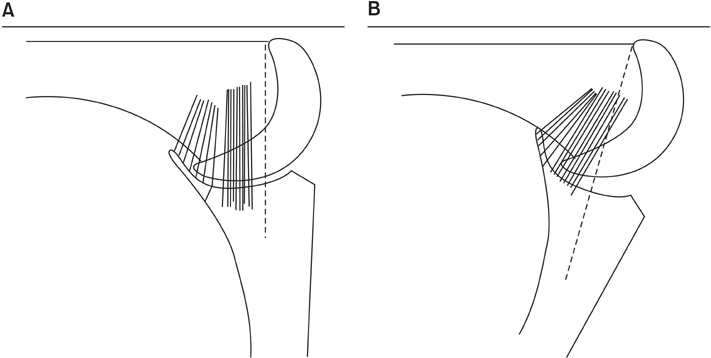
Fig. 5 Diagram of our ligament-preserving surgical approach to remove condylar osteophytes. (A) When the metacarpophalangeal joint (MPJ) is flexed at 90°, the distal half of the radial osteophyte can be approached. (B) If the MPJ is hyperflexed beyond 90°, the more proximal portion of the radial osteophyte can be approached.
Reference
-
1. Inoue G, Miura T. Locked metacarpophalangeal joint of the finger. Orthop Rev. 1991; 20(2):149–153.2. Thomsen L, Roulot E, Barbato B, Dumontier C. Locked metacarpophalangeal joint of long fingers: classification, definition and treatment based on 15 cases and literature review. Chir Main. 2011; 30(4):269–275.3. Yagi M, Yamanaka K, Yoshida K, Sato N, Inoue A. Successful manual reduction of locked metacarpophalangeal joints in fingers. J Bone Joint Surg Am. 2000; 82(3):366–371.4. Langenskiold A. Habitual locking of a meta-carpo-phalangeal joint by a collateral ligament, a rare cause of trigger finger. Acta Chir Scand. 1949; 99(1):73–78.5. Lee S, Yum JK, Kim JY. Locking of the metacarpophalangeal joint of the thumb with the radial collateral ligament rupture after stress radiography. Arch Orthop Trauma Surg. 2010; 130(2):237–239.6. Kim JK, Chung MS, Baek GH. Locked metacarpophalangeal joint of the index finger: consideration about the surgical approach. J Hand Surg Eur Vol. 2009; 34(2):278–280.7. Guly HR, Azam MA. Locked finger treated by manipulation: a report of three cases. J Bone Joint Surg Br. 1982; 64(1):73–75.8. Tajima K, Sato K, Sasaki T, Peimer CA. Vertical locking of the metacarpophalangeal joint in young adults. J Hand Surg Am. 2011; 36(9):1482–1485.9. Aston JN. Locked middle finger. J Bone Joint Surg Br. 1960; 42-B:75–79.10. Bloom MH, Bryan RS. Locked index finger caused by hyperflexion and entrapment of sesamoid bone. J Bone Joint Surg Am. 1965; 47(7):1383–1385.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extension Type Locked Metacarpophalangeal Joint of the Little Finger due to Hyperextension Injury
- Dorsal Dislocation of the Metacarpophalangeal Joint of the Index Finger: A Case Report
- Dislocations of the Metacarpophalangeal Joints of the Fingers: Report of 2 Cases
- Stener-Like Lesions in the Metacarpophalangeal Joint of the Fingers
- Dislocation of the Metacarpophalangeal Joint Hand: Report of Three Cases
