Unusual Presentation of Cerebral Cavernous Malformation
- Affiliations
-
- 1Department of Neurosurgery, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea. djlim@korea.ac.kr
- KMID: 2069253
- DOI: http://doi.org/10.7461/jcen.2015.17.3.257
Abstract
- Cerebral cavernous malformations (CMs) are vascular malformations of the central nervous system, which can be detected in the absence of any clinical symptoms. Nodules and cysts with mixed signal intensity and a peripheral hemosiderin rim are considered brain magnetic resonance imaging (MRI) findings typical of CMs. A 48-year-old man was admitted to our hospital because of abnormal MRI findings without significant neurological symptoms. A cyst with an internal fluid-fluid level was found in the left basal ganglia on the initial brain MRI. We decided to observe the natural course of the asymptomatic lesion with serial MRI follow-up. On MRI at the 5-month follow-up, the cystic mass was enlarged and showed findings consistent with those of cystic CM. Surgical resection was performed and the pathological diagnosis was CM. Our experience suggests that the initial presentation of a CM can be a pure cyst and neurosurgeons should consider the likelihood of CMs in cases of cystic cerebral lesions with intracystic hemorrhage.
MeSH Terms
Figure
-
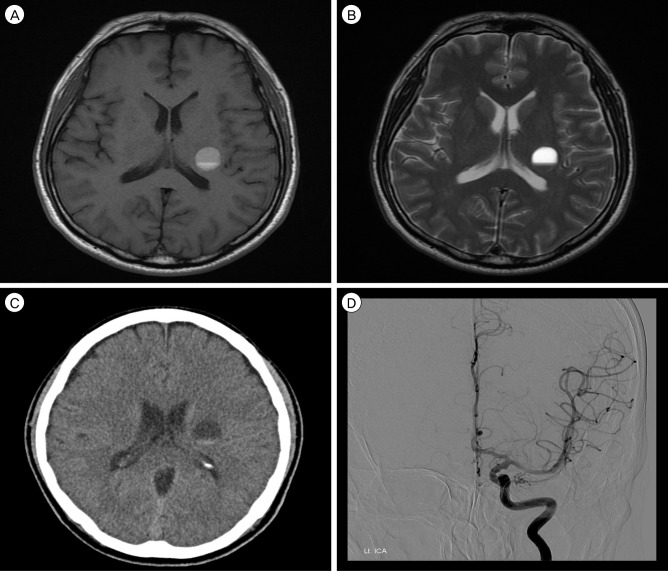
Fig. 1 Initial brain imaging findings for this patient. Axial T1-weighted (A), T2-weighted (B) magnetic resonance images, and computed tomography (C) showed a single cystic mass measuring 16 mm in diameter with a fluid-fluid level in the left basal ganglia. Note that there was no evidence of solid components or a hemosiderin rim. An angiogram (D) showed neither abnormal tumor staining nor vascular malformation.
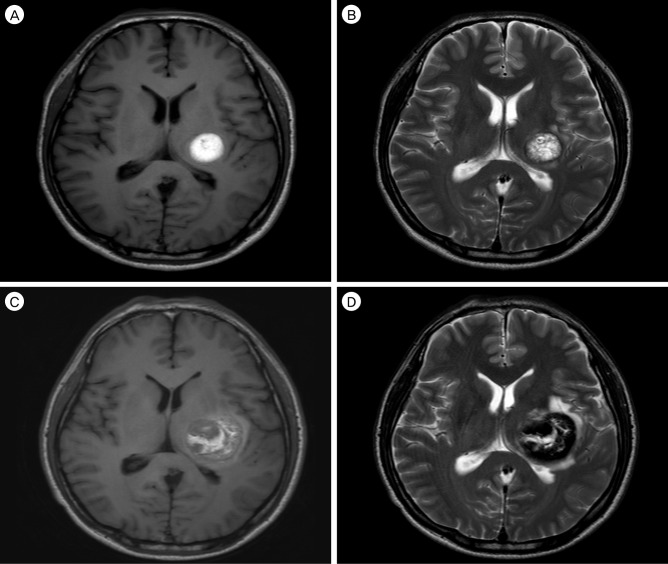
Fig. 2 First repeated brain imaging performed 5 months after the initial studies (A and B) and preoperative imaging performed 7 months after the initial studies (C and D). Axial T1-weighted (A), T2-weighted (B) magnetic resonance images showed a reticulated "salt and pepper" pattern in the core and a peripheral halo of low signal intensity. Axial T1-weighted (C), and T2-weighted (D) magnetic resonance images showed an increase in the size of the lesion with aggravated peri-lesional edema. Mixed signal intensity in the core with peripheral low signal intensity gradually becomes more distinct.
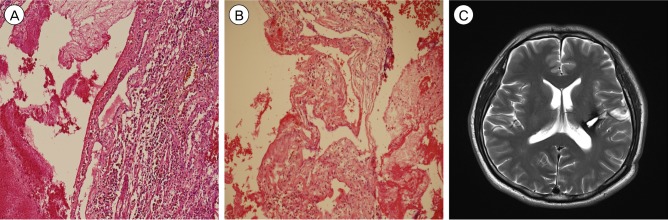
Fig. 3 In the histopathological examination, the lesion showed irregularly dilated vascular channels lacking a smooth muscle layer. A rim of fibrosis and hemosiderin-laden macrophages on a hemorrhagic background surrounded the lesion. In the lumen of the vascular channels, there were some organizing thrombi. However, there was no evidence of microcalcification. These histopathological findings were consistent with CM. Hematoxylin-eosin staining; magnification ×100 (A and B). A post-operative axial T2-weighted magnetic resonance image (C) shows no residual lesion.
Reference
-
1. Aiba T, Tanaka R, Koike T, Kameyama S, Takeda N, Komata T. Natural history of intracranial cavernous malformations. J Neurosurg. 1995; 7. 83(1):56–59. PMID: 7782850.
Article2. Bertalanffy H, Benes L, Miyazawa T, Alberti O, Siegel AM, Sure U. Cerebral cavernomas in the adult: review of the literature and analysis of 72 surgically treated patients. Neurosurg Rev. 2002; 3. 25(1-2):1–53. discussion 54-5PMID: 11954761.
Article3. Flemming KD, Link MJ, Christianson TJ, Brown RD. Prospective hemorrhage risk of intracerebral cavernous malformations. Neurology. 2012; 2. 78(9):632–636. PMID: 22302553.
Article4. Gross BA, Lin N, Du R, Day AL. The natural history of intracranial cavernous malformations. Neurosurg Focus. 2011; 6. 30(6):E24. PMID: 21631226.
Article5. Hatachita S, Miyajima M, Koga N. Cystic cavernous angioma-case report. Neurol Med Chir (Tokyo). 1991; 7. 31(7):414–416. PMID: 1720221.6. Kadota O, Sakaki S, Kumon Y, Ohta S, Kohno K. Large cystic cavernous angioma of the cerebellum: case report. Neurol Med Chir (Tokyo). 1994; 11. 34(11):768–772. PMID: 7533273.
Article7. Kim IC, Kwon KY, Rhee JJ, Lee JW, Hur JW, Lee HK. Giant cystic cerebral cavernous malformation with multiple calcification: case report. J Cerebrovasc Endovasc Neurosurg. 2013; 9. 15(3):255–259. PMID: 24167810.8. Kondziolka D, Lunsford LD, Kestle JR. The natural history of cerebral cavernous malformations. J Neurosurg. 1995; 11. 83(5):820–824. PMID: 7472549.
Article9. Lehnhardt FG, vonSmekal U, Rückriem B, Stenzel W, Neveling M, Heiss WD, et al. Value of gradient-echo magnetic resonance imaging in the diagnosis of familial cerebral cavernous malformation. Arch Neurol. 2005; 4. 62(4):653–658. PMID: 15824268.
Article10. Mathiesen T, Edner G, Kihlström L. Deep and brainstem cavernomas: a consecutive 8-year series. J Neurosurg. 2003; 7. 99(1):31–37. PMID: 12854740.
Article11. Ohba S, Shimizu K, Shibao S, Nakagawa T, Murakami H. Cystic cavernous angiomas. Neurosurg Rev. 2010; 10. 33(4):395–400. PMID: 20174956.
Article12. Osborn AG, Preece MT. Intracranial cysts: radiologicpathologic correlation and imaging approach. Radiology. 2006; 6. 239(3):650–664. PMID: 16714456.
Article13. Pandey P, Westbroek EM, Gooderham PA, Steinberg GK. Cavernous malformation of brainstem, thalamus and basal ganglia: a series of 176 patients. Clinical studies. Neurosurgery. 2013; 4. 72(4):573–589. discussion 588-9PMID: 23262564.14. Poorthuis MH, Klijn CJ, Algra A, Rinkel GJ, Al-Shahi Salman R. Treatment of cerebral cavernous malformations: a systematic review and meta-regression analysis. J Neurol Neurosurg Psychiatry. 2014; 12. 85(12):1319–1323. PMID: 24667206.
Article15. Porter PJ, Willinsky RA, Harper W, Wallace MC. Cerebral cavernous malformations: natural history and prognosis after clinical deterioration with or without hemorrhage. J Neurosurg. 1997; 8. 87(2):190–197. PMID: 9254081.
Article16. Ramina R, Ingunza W, Vonofakos D. Cystic cerebral cavernous angioma with dense calcification: case report. J Neurosurg. 1980; 2. 52(2):259–262. PMID: 7351568.17. Robinson JR, Awad IA, Little JR. Natural history of the cavernous angioma. J Neurosurg. 1991; 11. 75(5):709–714. PMID: 1919692.
Article18. Al-Shahi Salman R, Hall JM, Horne MA, Moultrie F, Josephson CB, Bhattacharya JJ, et al. Untreated clinical course of cerebral cavernous malformations: a prospective, population-based cohort study. Lancet Neurol. 2012; 3. 11(3):217–224. PMID: 22297119.19. Samii M, Eghbal R, Carvalho GA, Matthies C. Surgical management of brainstem cavernomas. J Neurosurg. 2001; 11. 95(5):825–832. PMID: 11702873.
Article20. Sandalcioglu I, Wiedemayer H, Secer S, Asgari S, Stolke D. Surgical removal of brain stem cavernous malformations: surgical indications, technical considerations, and results. J Neurol Neurosurg Psychiatry. 2002; 3. 72(3):351–355. PMID: 11861694.
Article21. Sato K, Kubota T. Large calcified cystic cavernous angioma in the thalamus. Neurol Med Chir (Tokyo). 1995; 2. 35(2):100–103. PMID: 7753307.22. Siddiqui AA, Jooma R. Neoplastic growth of cerebral cavernous malformation presenting with impending cerebral herniation: a case report and review of the literature on de novo growth of cavernomas. Surg Neurol. 2001; 7. 56(1):42–45. PMID: 11546573.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case involving anesthesia for cesarean section followed by resection of ruptured cavernous malformation of pons :A case report
- A Case of Orbital Cavernous Angioma Associated with Intracranial Venous Anomalies
- Cavernous Hemangioma on the Frontal Lobe
- Pathophysiology of Cerebral Arteiovenous Malformation
- A Case of Cavernous Angioma of the Cerebellar Vermis
