Sex Differences in Remifentanil Requirements for Preventing Cough during Anesthetic Emergence
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Yonsei University College of Medicine, Seoul, Korea. leejeongrim@gmail.com
- 2Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Surgery, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2068695
- DOI: http://doi.org/10.3349/ymj.2014.55.3.807
Abstract
- PURPOSE
Target-controlled infusion (TCI) of remifentanil can suppress coughing during emergence from general anesthesia; nevertheless, previous studies under different clinical conditions recommend significantly different effective effect-site concentrations (effective Ce) of remifentanil for 50% of patients (EC50). The differences among these studies include type of surgery and patient sex. In recent years, study of sex differences in regards to anesthetic pharmacology has drawn greater interest. Accordingly, we attempted to determine the effective Ce of remifentanil for preventing cough for each sex under the same clinical conditions.
MATERIALS AND METHODS
Twenty female and 25 male ASA physical status I-II grade patients between the ages of 20 and 46 years who were undergoing thyroidectomy were enrolled in this study. The effective Ce of remifentanil for preventing cough was determined for each sex using the isotonic regression method with a bootstrapping approach, following Dixon's up-and-down method.
RESULTS
Isotonic regression with a bootstrapping approach revealed that the estimated EC50 of remifentanil for preventing coughing during emergence was significantly lower in females {1.30 ng/mL [83% confidence interval (CI), 1.20-1.47 ng/mL]} than in males [2.57 ng/mL (83% CI, 2.45-2.70 ng/mL)]. Mean EC50 in females was also significantly lower than in males (1.23+/-0.21 ng/mL vs. 2.43+/-0.21 ng/mL, p<0.001). Mean arterial pressure, heart rate, and respiratory rate over time were not significantly different between the sexes.
CONCLUSION
When using remifentanil TCI for cough prevention during anesthetic emergence, patient sex should be a considered for appropriate dosing.
Keyword
MeSH Terms
Figure
-
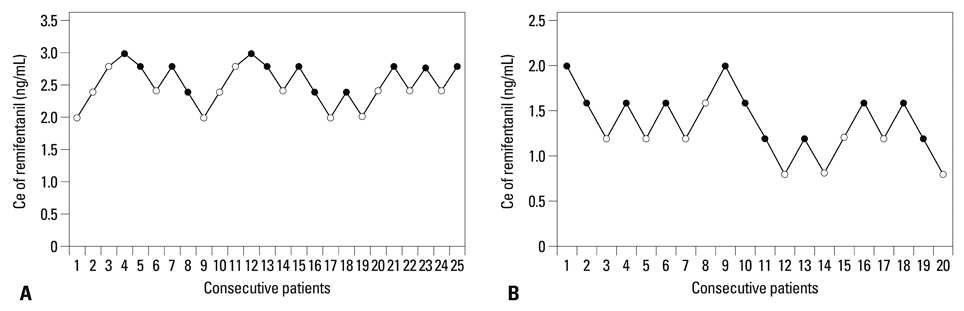
Fig. 1 Assessment of success or failure of smooth emergence over the predetermined concentration of remifentanil based on consecutive patients by Dixon's up-and-down method. Mean EC50 for smooth emergence was calculated from cross-over pairs from failure (open circle) to success (closed circle) in 25 male patients (A) and 20 female patients (B). EC50, effective effect-site concentration (Ce) of remifentanil for suppression of emergence cough in 50% of patients.
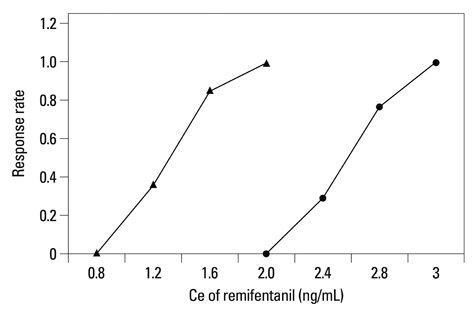
Fig. 2 Pooled-adjacent-violators algorithm response rate in female (▲) and male (●) groups. EC50 of remifentanil in females was 1.30 ng/mL (83% CI, 1.20-1.47 ng/mL) and 2.57 ng/mL (83% CI, 2.45-2.70 ng/mL) in males. EC95 in females was 1.86 ng/mL (95% CI, 1.56-1.96 ng/mL) and 2.96 ng/mL (95% CI, 2.77-2.98 ng/mL) in males. Both EC50 and EC95 were significantly lower in the female group than in the male group. EC50, effective Ce of remifentanil for suppression of emergence cough in 50% of patients; EC95, effective Ce of remifentanil for suppression of emergence cough in 95% of patients; CI, confidence interval.
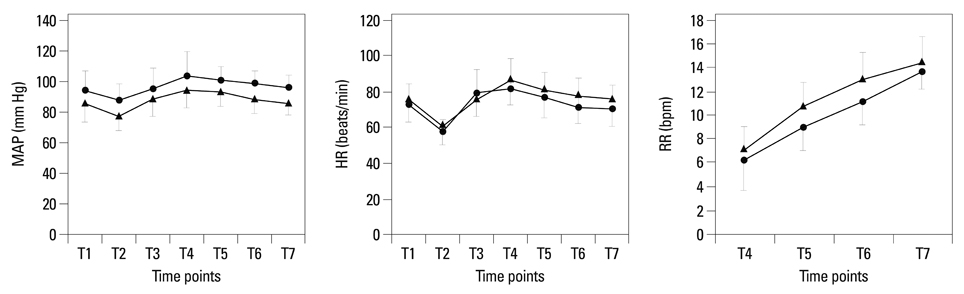
Fig. 3 MAP, HR, and RR were not significantly different in females (▲) and males (●) over time (p-values for MAP, HR, and RR=0.351, 0.082 and 0.277, respectively). The female MAP was significantly higher than that of males at the end of the surgery, 10 min after extubation, and before transfer out from the postanesthetic care unit (p=0.012, p<0.001, and p<0.001, respectively). With regard to HR, there was no significant difference at any time point. RR increased continuously from each prior time point in both males and females: just after extubation to 5 min after extubation (p<0.001), 5 min after extubation to10 min after extubation (p<0.001), and 10 min after extubation to before transfer out from the post-anesthetic care unit (p<0.001). MAP, mean arterial pressure; HR, heart rate; RR, respiratory rate; bpm, breaths per min.
Reference
-
1. Miller KA, Harkin CP, Bailey PL. Postoperative tracheal extubation. Anesth Analg. 1995; 80:149–172.2. Soltani HA, Aghadavoudi O. The effect of different lidocaine application methods on postoperative cough and sore throat. J Clin Anesth. 2002; 14:15–18.
Article3. Kim ES, Bishop MJ. Cough during emergence from isoflurane anesthesia. Anesth Analg. 1998; 87:1170–1174.4. Lee HS, Lee BJ, Kim SW, Cha YW, Choi YS, Park YH, et al. Patterns of Post-thyroidectomy Hemorrhage. Clin Exp Otorhinolaryngol. 2009; 2:72–77.
Article5. Godballe C, Madsen AR, Pedersen HB, Sørensen CH, Pedersen U, Frisch T, et al. Post-thyroidectomy hemorrhage: a national study of patients treated at the Danish departments of ENT Head and Neck Surgery. Eur Arch Otorhinolaryngol. 2009; 266:1945–1952.
Article6. Leyre P, Desurmont T, Lacoste L, Odasso C, Bouche G, Beaulieu A, et al. Does the risk of compressive hematoma after thyroidectomy authorize 1-day surgery? Langenbecks Arch Surg. 2008; 393:733–737.
Article7. Harding J, Sebag F, Sierra M, Palazzo FF, Henry JF. Thyroid surgery: postoperative hematoma--prevention and treatment. Langenbecks Arch Surg. 2006; 391:169–173.
Article8. Chen J, Li W, Wang D, Hu X. The effect of remifentanil on cough suppression after endoscopic sinus surgery: a randomized study. Acta Anaesthesiol Scand. 2010; 54:1197–1203.
Article9. Tagaito Y, Isono S, Nishino T. Upper airway reflexes during a combination of propofol and fentanyl anesthesia. Anesthesiology. 1998; 88:1459–1466.
Article10. Kim JM, Lee JH, Lee HJ, Koo BN. Comparison of emergence time in children undergoing minor surgery according to anesthetic: desflurane and sevoflurane. Yonsei Med J. 2013; 54:732–738.
Article11. Nishina K, Mikawa K, Maekawa N, Obara H. Fentanyl attenuates cardiovascular responses to tracheal extubation. Acta Anaesthesiol Scand. 1995; 39:85–89.
Article12. Egan TD. Target-controlled drug delivery: progress toward an intravenous "vaporizer" and automated anesthetic administration. Anesthesiology. 2003; 99:1214–1219.13. Lee B, Lee JR, Na S. Targeting smooth emergence: the effect site concentration of remifentanil for preventing cough during emergence during propofol-remifentanil anaesthesia for thyroid surgery. Br J Anaesth. 2009; 102:775–778.
Article14. Choi EM, Park WK, Choi SH, Soh S, Lee JR. Smooth emergence in men undergoing nasal surgery: the effect site concentration of remifentanil for preventing cough after sevoflurane-balanced anaesthesia. Acta Anaesthesiol Scand. 2012; 56:498–503.
Article15. Fillingim RB, Gear RW. Sex differences in opioid analgesia: clinical and experimental findings. Eur J Pain. 2004; 8:413–425.
Article16. Dahan A, Kest B, Waxman AR, Sarton E. Sex-specific responses to opiates: animal and human studies. Anesth Analg. 2008; 107:83–95.
Article17. Sarton E, Olofsen E, Romberg R, den Hartigh J, Kest B, Nieuwenhuijs D, et al. Sex differences in morphine analgesia: an experimental study in healthy volunteers. Anesthesiology. 2000; 93:1245–1254.18. Dahan A, Sarton E, Teppema L, Olievier C. Sex-related differences in the influence of morphine on ventilatory control in humans. Anesthesiology. 1998; 88:903–913.
Article19. Kamei J. Role of opioidergic and serotonergic mechanisms in cough and antitussives. Pulm Pharmacol. 1996; 9:349–356.
Article20. Minto CF, Schnider TW, Egan TD, Youngs E, Lemmens HJ, Gambus PL, et al. Influence of age and gender on the pharmacokinetics and pharmacodynamics of remifentanil I Model development. Anesthesiology. 1997; 86:10–23.
Article21. Dixon WJ. Staircase bioassay: the up-and-down method. Neurosci Biobehav Rev. 1991; 15:47–50.
Article22. Pace NL, Stylianou MP. Advances in and limitations of up-and-down methodology: a précis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007; 107:144–152.23. Stylianou M, Flournoy N. Dose finding using the biased coin up-and-down design and isotonic regression. Biometrics. 2002; 58:171–177.
Article24. Dilleen M, Heimann G, Hirsch I. Non-parametric estimators of a monotonic dose-response curve and bootstrap confidence intervals. Stat Med. 2003; 22:869–882.
Article25. Payton ME, Greenstone MH, Schenker N. Overlapping confidence intervals or standard error intervals: what do they mean in terms of statistical significance? J Insect Sci. 2003; 3:34.
Article26. Jun NH, Lee JW, Song JW, Koh JC, Park WS, Shim YH. Optimal effect-site concentration of remifentanil for preventing cough during emergence from sevoflurane-remifentanil anaesthesia. Anaesthesia. 2010; 65:930–935.
Article27. Dicpinigaitis PV, Rauf K. The influence of gender on cough reflex sensitivity. Chest. 1998; 113:1319–1321.
Article28. Andrade J, Sapsford DJ, Jeevaratnum D, Pickworth AJ, Jones JG. The coherent frequency in the electroencephalogram as an objective measure of cognitive function during propofol sedation. Anesth Analg. 1996; 83:1279–1284.
Article29. Glass PS, Bloom M, Kearse L, Rosow C, Sebel P, Manberg P. Bispectral analysis measures sedation and memory effects of propofol, midazolam, isoflurane, and alfentanil in healthy volunteers. Anesthesiology. 1997; 86:836–847.
Article30. Li Y, Zhou Y, Chen H, Feng Z. The effect of sex on the minimum local analgesic concentration of ropivacaine for caudal anesthesia in anorectal surgery. Anesth Analg. 2010; 110:1490–1493.
Article31. Semple P, Hope DA, Clyburn P, Rodbert A. Relative potency of vecuronium in male and female patients in Britain and Australia. Br J Anaesth. 1994; 72:190–194.
Article32. Xue FS, Liao X, Liu JH, Tong SY, Zhang YM, Zhang RJ, et al. Dose-response curve and time-course of effect of vecuronium in male and female patients. Br J Anaesth. 1998; 80:720–724.
Article33. Xue FS, Tong SY, Liao X, Liu JH, An G, Luo LK. Dose-response and time course of effect of rocuronium in male and female anesthetized patients. Anesth Analg. 1997; 85:667–671.
Article34. Burns JW, Hodsman NB, McLintock TT, Gillies GW, Kenny GN, McArdle CS. The influence of patient characteristics on the requirements for postoperative analgesia. A reassessment using patient-controlled analgesia. Anaesthesia. 1989; 44:2–6.
Article35. Chia YY, Chow LH, Hung CC, Liu K, Ger LP, Wang PN. Gender and pain upon movement are associated with the requirements for postoperative patient-controlled iv analgesia: a prospective survey of 2,298 Chinese patients. Can J Anaesth. 2002; 49:249–255.
Article36. Pleym H, Spigset O, Kharasch ED, Dale O. Gender differences in drug effects: implications for anesthesiologists. Acta Anaesthesiol Scand. 2003; 47:241–259.
Article37. Zubieta JK, Dannals RF, Frost JJ. Gender and age influences on human brain mu-opioid receptor binding measured by PET. Am J Psychiatry. 1999; 156:842–848.
Article38. Zubieta JK, Smith YR, Bueller JA, Xu Y, Kilbourn MR, Jewett DM, et al. mu-opioid receptor-mediated antinociceptive responses differ in men and women. J Neurosci. 2002; 22:5100–5107.
Article39. Mertens MJ, Engbers FH, Burm AG, Vuyk J. Predictive performance of computer-controlled infusion of remifentanil during propofol/remifentanil anaesthesia. Br J Anaesth. 2003; 90:132–141.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The effect of remifentanil infusion on coughing during emergence from general anesthesia with desflurane
- The effect of a subhypnotic dose of propofol for the prevention of coughing in adults during emergence from anesthesia with sevoflurane and remifentanil
- The Effects of Anesthetic Agents on Emergence Delirium in Pediatric Strabismus Surgery
- Fentanyl versus Remifentanil for Cough Suppression and Recovery after Video-Assisted Thoracic Surgery
- The clinical effective dose of alfentanil for suppressing cough during emergence from desflurane anesthesia
