J Korean Neurosurg Soc.
2012 May;51(5):305-307. 10.3340/jkns.2012.51.5.305.
Sixth and Twelfth Cranial Nerve Palsies Following Basal Skull Fracture Involving Clivus and Occipital Condyle
- Affiliations
-
- 1Department of Rehabilitation, Wonju College of Medicine, Younsei University, Wonju, Korea.
- 2Department of Neurosurgery, School of Medicine, Chosun University, Gwangju, Korea. chosunns@hanmail.net
- KMID: 2066932
- DOI: http://doi.org/10.3340/jkns.2012.51.5.305
Abstract
- Oblique basal skull fractures resulting from lateral crushing injuries involving both clivus and occipital condyle are rare due to their deep locations. Furthermore, these fractures may present clinically with multiple cranial nerve injuries because neural exit routes are restricted in this intricate region. The authors present an interesting case of basal skull fractures involving the clivus and occipital condyle and presenting with sixth and contralateral twelfth cranial nerve deficits. Clinico-anatomic correlations and the courses of cranial nerve deficits are reiterated. To the authors' knowledge, no other report has been previously issued on concomitant sixth and contralateral twelfth cranial nerve palsies following closed head injury.
Keyword
MeSH Terms
Figure
-

Fig. 1 Detailed neurological examination of the patient. A : Patient shows right VI nerve palsy with restriction of lateral gaze. B : Patient shows left XII nerve palsy with tongue deviation.
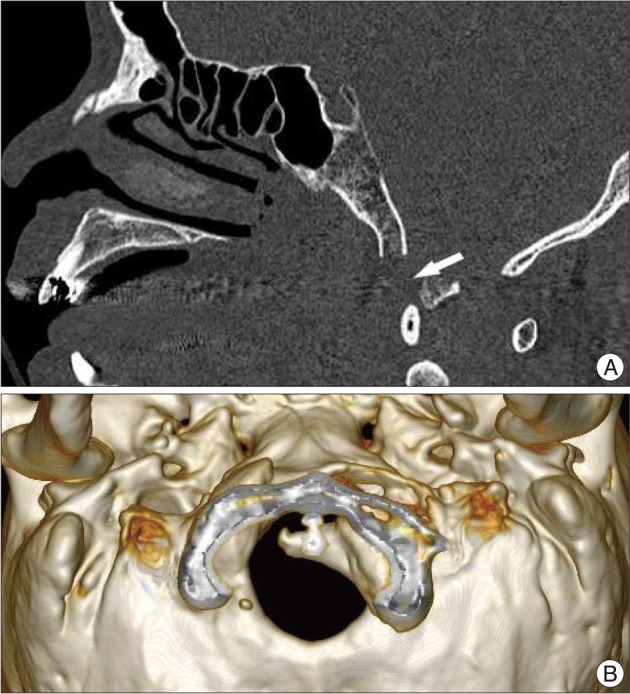
Fig. 2 Computed tomographic scan of the patient. A : Sagittal computed scan (bone window) shows clivus fracture. B : Three dimensional computed scan reveals an avulsion fracture of the occipital condyle depressed around the foramen magnum.
Reference
-
1. Anderson PA, Montesano PX. Morphology and treatment of occipital condyle fractures. Spine (Phila Pa 1976). 1988; 13:731–736. PMID: 3194779.
Article2. Dagi TF, George ED. Schnideck HH, Sweet WH, editors. Surgical management of cranial cerebrospinal fluid fistulas. Operative Neurosurgical Techniques. 1995. Philadelphia: WB Saunders;p. 117–131.3. Dhaliwal A, West AL, Trobe JD, Musch DC. Third, fourth, and sixth cranial nerve palsies following closed head injury. J Neuroophthalmol. 2006; 26:4–10. PMID: 16518159.
Article4. Jennett B, Teasdale G, Fry J, Braakman R, Minderhoud J, Heiden J, et al. Treatment for severe head injury. J Neurol Neurosurg Psychiatry. 1980; 43:289–295. PMID: 6768847.
Article5. Kerman M, Cirak B, Dagtekin A. Management of skull base fractures. Neurosurg Q. 2002; 12:23–41.
Article6. Khan N, Zumstein B. Transverse clivus fracture : case presentation and significance of clinico-anatomic correlations. Surg Neurol. 2000; 54:171–177. PMID: 11077100.
Article7. Lee YS, Song SH, Kim SH, Kim KT, Kim Y. Clinical analysis of basal skull fractures. J Korean Neurosurg Soc. 1994; 23:1038–1046.8. Menkü A, Koç RK, Tucer B, Durak AC, Akdemir H. Clivus fractures : clinical presentations and courses. Neurosurg Rev. 2004; 27:194–198. PMID: 15034764.9. Ommaya AK. Wilkins RH, Rengachary SS, editors. Cerebrospinal fluid fistula and pneumocephalus. Neurosurgery. 1996. Vol 2:ed 2. New York: McGraw-Hill;p. 2773–2782.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Collet-Sicard Syndrome Associated with Occipital Condyle Fracture and Epidural Hematoma
- Sixth Cranial Nerve Palsy Caused by Gastric Adenocarcinoma Metastasis to the Clivus
- Delayed Hypoglossal Nerve Palsy Following Fracture of the Occipital Condyle: Case Report
- A Case of Occipital Condyle Syndrome Associated with Hepatocellular Carcinoma
- Management of a traumatic avulsion fracture of the occipital condyle in polytrauma patient in Korea: a case report
