J Korean Endocr Soc.
2008 Feb;23(1):51-55. 10.3803/jkes.2008.23.1.51.
A Case of Unilateral Exophthalmos Caused by a Dural Arteriovenous Malformation in Thyroid-Associated Ophthalmopathy
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Hallym University, Korea.
- KMID: 2063550
- DOI: http://doi.org/10.3803/jkes.2008.23.1.51
Abstract
- Thyroid-associated ophthalmopathy is associated with thyroid dysfunction, particularly Graves' disease, and is manifested as eye signs, including proptosis. In cases of unilateral exophthalmos with thyroid-associated ophthalmopathy, other causes such as orbital neoplasm, carotid-cavernous fistula, cavernous sinus thrombosis, and dural arteriovenous malformation (AVM) should be excluded. Dural AVM, an abnormal dural arteriovenous connection, is a rare neurovascular entity that mimics thyroid-associated ophthalmopathy. When eye involvement is unilateral or asymmetric, dural AVM can be considered in the differential diagnosis of thyroid-associated ophthalmopathy. A twenty-six year-old woman presented with unilateral exophthalmos in Graves' disease. By orbital magnetic resonance imaging and cerebral angiography, thyroid-associated ophthalmopathy and dural AVM were diagnosed. The unilateral exophthalmos improved after coil embolization of the dural AVM. In summary, we report the first case of a dural AVM with Graves' disease and thyroid-associated ophthalmopathy.
MeSH Terms
Figure
-

Fig. 1 Orbital MRI. Right exophthalmos, both extraocular muscle thickening and right retro-orbital vessel engorgement (arrow) are seen.
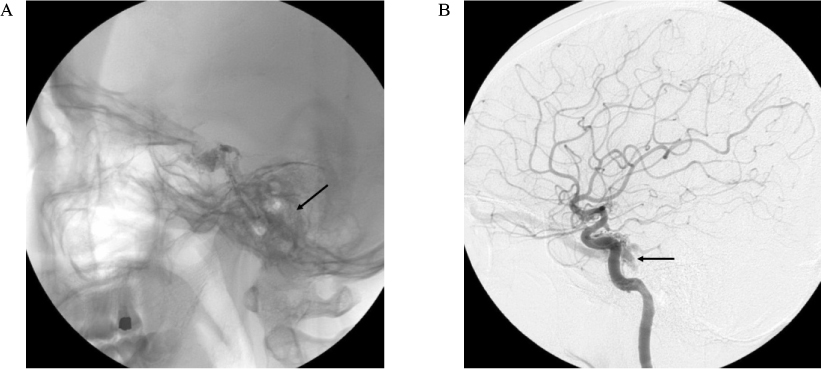
Fig. 2 Cerebral angiography reveals dural arteriovenous malformation (AVM) without cortical venous reflex, so called type I AVM (arrows).

Fig. 3 After selection of dural AVM, coil embolization was performed in abnormal vessel.
Reference
-
1. Bartalena L, Pinchera A, Marcocci C. Management of Graves' ophthalmopathy: reality and perspectives. Endocr Rev. 2000. 21:168–199.2. Prabhakar BS, Bahn RS, Smith TJ. Current perspective on the pathogenesis of Graves' disease and ophthalmopathy. Endocr Rev. 2003. 24:802–835.3. Burch HB, Wartofsky L. Graves' ophthalmopathy: current concepts regarding pathogenesis and management. Endocr Rev. 1993. 14:747–793.4. Drescher EP, Benedict WL. Asymmetric exophthalmos. Arch Ophthal. 1950. 44:109–128.5. DeSanto LW. The total rehabilitation of Graves' ophthalmopathy. Laryngoscope. 1980. 90:1652–1678.6. Loré F, Polito E, Cerase A, Bracco S, Loffredo A, Pichierri P, Talidis F. Carotid cavernous fistula in a patient with Graves' ophthalmopathy. J Clin Endocrinol Metab. 2003. 88:3487–3490.7. Werner SC. Classification of the eye changes Graves' disease. J Clin Endocrinol Metab. 1969. 29:982–984.8. Mourits MP, Koornneef L, Wiersinga WM, Prummel MF, Berghout A, van der Gaag R. Clinical criteria for the assessment of disease activity in Graves' ophthalmopathy: a novel approach. Br J Ophthalmol. 1989. 73:639–644.9. The European Group on Graves' Orbitopathy. Clinical assessment of patients with Graves' orbitopathy: the European Group on Graves' Orbitopathy recommendations to generalists, specialists and clinical researchers. Eur J Endocrinol. 2006. 155:387–389.10. Enzmann DR, Donaldson SS, Kriss JP. Appearance of Graves' disease on orbital computed tomography. J Comput Assist Tomogr. 1979. 3:815–819.11. Wiersinga WM, Smit T, van der Gaag R, Mourits M, Koornneef L. Clinical presentation of Graves' ophthalmopathy. Ophthalmic Res. 1989. 21:73–82.12. Forbes G, Gorman CA, Brennan MD, Gehring DG, Ilstrup DM, Earnest F 4th. Ophthalmopathy of Graves' disease: computerized volume measurements of the orbital fat and muscle. AJNR Am J Neuroradiol. 1986. 7:651–656.13. Fledelius HC, Glydensted C. Ultrasonography and computed tomography in orbital diagnosis: with special reference to dysthyroid ophthalmopathy. Acta Ophthalmol(Copenh). 1978. 56:751–762.14. Dallow RL. Evaluation of unilateral exophthalmos with ultrasonography: analysis of 258 consecutive cases. Laryngoscope. 1975. 85:1905–1919.15. Kahaly GJ. Imaging in thyroid-associated orbitopathy. Eur J Endocrinol. 2001. 145:107–118.16. Kerber CW, Newton TH. The macro and microvasculature of the dura mater. Neuroradiology. 1973. 6:175–179.17. Awad IA, Little JR, Akarawi WP, Ahl J. Intracranial dural arteriovenous malformations: factors predisposing to an aggressive neurological course. J Neurosurg. 1990. 72:839–850.18. Lawton MT, Jacobowitz R, Spetzler RF. Redefined role of angiogenesis in the pathogenesis of dural arteriovenous malformations. J Neurosurg. 1997. 87:267–274.19. Kiyosue H, Hori Y, Okahara M, Tanoue S, Sagara Y, Matsumoto S, Nagatomi H, Mori H. Treatment of intracranial dural arteriovenous fistulas: current strategies based on location and hemodynamics, and alternative techniques of transcatheter embolization. Radiographics. 2004. 24:1637–1653.20. Borden JA, Wu JK, Shucart WA. A proposed classification for spinal and cranial dural arteriovenous fistulous malformations and implications for treatment. J Neurosurg. 1995. 82:166–179.21. Houser OW, Baker HL Jr, Rhoton AL Jr, Okazaki H. Intracranial dural arteriovenous malformations. Radiology. 1972. 105:55–64.22. Djindjian R, Merland J. Meningeal arteriovenous fistula. Superselective arteriography of the external carotid artery. 1978. New York: Springer-Verlag;405–406.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dural Arteriovenous Malformation Associated with Meningioma: Spontaneous Disappearance after Tumor Removal: Case Report
- A Case of Graves' Disease Showing a Triad of Ophthalmopathy, Pretibial Myxedema and Thyroid Acropachy
- Endovascular Treatment of Dural Sinus Malformation in Infant: A Case Report
- A Case of Mixed Pial and Dural Arteriovenous Malformation in the Left Frontal Convexity
- Three Wall Orbital Decompression for Compressive Optic Neuropathy in Thyroid Ophthalmopathy
