Obstet Gynecol Sci.
2015 Sep;58(5):427-430. 10.5468/ogs.2015.58.5.427.
Massive hemoperitoneum due to a ruptured corpus luteum cyst in a patient with congenital hypofibrinogenemia
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Institute for Medical Sciences, Chonbuk National University Medical School, Jeonju, Korea. obgyn2001@jbnu.ac.kr
- KMID: 2058471
- DOI: http://doi.org/10.5468/ogs.2015.58.5.427
Abstract
- Congenital afibrinogenemia/hypofibrinogenemia is a rare inherited hematologic disorder in which a patient lacks or has insufficient level of fibrinogen, the blood coagulation factor I. The incidence of this uncommon disease is 1 to 2 per 1 million individuals. Hence, massive hemoperitoneum caused by ovulation in a woman with congenital afibrogenemia is also a very rare clinical condition. Massive hemoperitoneum usually presents as acute abdominal pain with potential findings of peritonitis including abdominal distention, hypotension and tachycardia with critical consequences. We performed emergent endoscopic surgery for hemoperitoneum caused by a ruptured corpus luteum cyst in a patient with congenital hypofibrinogenemia. To the best of our knowledge, this was the first case report of such treatment in Korea.
MeSH Terms
Figure
-
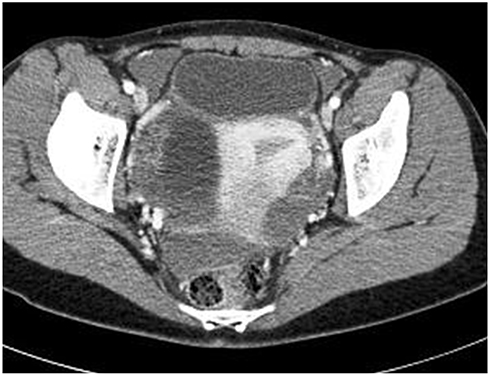
Fig. 1 Computed tomography image shows ruptured corpus luteum cyst of right ovary and huge amount of hemoperitoneum in pelvic cavity around uterus.
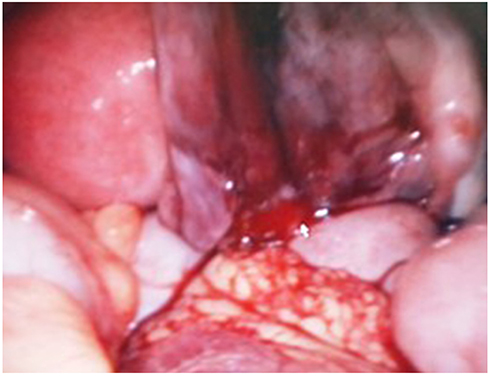
Fig. 2 Intraoperative findings: the focus of bleeding from ruptured site of corpus luteum cyst of right ovary.
Reference
-
1. Asselta R, Duga S, Tenchini ML. The molecular basis of quantitative fibrinogen disorders. J Thromb Haemost. 2006; 4:2115–2129.2. Acharya SS, Coughlin A, Dimichele DM. North American Rare Bleeding Disorder Study Group. Rare Bleeding Disorder Registry: deficiencies of factors II, V, VII, X, XIII, fibrinogen and dysfibrinogenemias. J Thromb Haemost. 2004; 2:248–256.3. Mannucci PM, Duga S, Peyvandi F. Recessively inherited coagulation disorders. Blood. 2004; 104:1243–1252.4. Peyvandi F, Haertel S, Knaub S, Mannucci PM. Incidence of bleeding symptoms in 100 patients with inherited afibrinogenemia or hypofibrinogenemia. J Thromb Haemost. 2006; 4:1634–1637.5. Lucey BC, Varghese JC, Soto JA. Spontaneous hemoperitoneum: causes and significance. Curr Probl Diagn Radiol. 2005; 34:182–195.6. Keeling D, Tait C, Makris M. Guideline on the selection and use of therapeutic products to treat haemophilia and other hereditary bleeding disorders. A United Kingdom Haemophilia Center Doctors' Organisation (UKHCDO) guideline approved by the British Committee for Standards in Haematology. Haemophilia. 2008; 14:671–684.7. Bolton-Maggs PH, Perry DJ, Chalmers EA, Parapia LA, Wilde JT, Williams MD, et al. The rare coagulation disorders--review with guidelines for management from the United Kingdom Haemophilia Centre Doctors' Organisation. Haemophilia. 2004; 10:593–628.8. Oruc N, Tokat Y, Killi R, Tombuloglu M, Ilter T. Budd-Chiari syndrome in an afibrinogenemic patient: a paradoxical complication. Dig Dis Sci. 2006; 51:378–380.9. Bottini E, Pareti FI, Mari D, Mannucci PM, Muggiasca ML, Conti M. Prevention of hemoperitoneum during ovulation by oral contraceptives in women with type III von Willebrand disease and afibrinogenemia. Case reports. Haematologica. 1991; 76:431–433.10. Castaman G, Ruggeri M, Rodeghiero F. Congenital afibrinogenemia: successful prevention of recurrent hemoperitoneum during ovulation by oral contraceptive. Am J Hematol. 1995; 49:363–364.
