Captured Macro-embolus of Fractured Atheromatous Plaque by the Embolic Protection Device during Carotid Stent Assisted Angioplasty
- Affiliations
-
- 1Department of Radiology, The University of Chicago, Chicago, IL, USA. sklee@uchicago.edu
- 2Department of Neurosurgery, Pohang Stroke and Spine Hospital, Pohang, Korea.
- 3Department of Medical Imaging, Toronto Western Hospital, Toronto, ON, Canada.
- 4Department of Pathology, Toronto Western Hospital, Toronto, ON, Canada.
- KMID: 2052082
- DOI: http://doi.org/10.5469/neuroint.2013.8.1.52
Abstract
- The authors present a case in which macro-embolus from the ruptured atheromatous plaque developed during carotid artery stenting (CAS). A 63-year-old man who had suffered a left middle cerebral artery territory infarction had significant proximal left internal carotid artery stenosis required CAS procedure. Immediate after stent deployment, the patient showed abrupt neurological deterioration with 12 x 3 mm sized macro-embolus which was caught by the embolus protection device (EPD). Retrieval of the macro-embolus was performed safely and the patient recovered to pre-procedure status. Macro-embolus can be resulted during the CAS. The EPD can capture the macro-embolus and safe removal is technically feasible.
MeSH Terms
Figure
-

Fig. 1 Lateral view of the left CCA angiogram shows about 70% of smooth luminal stenosis without angiographic evidence plaque ulcer or irregularity.
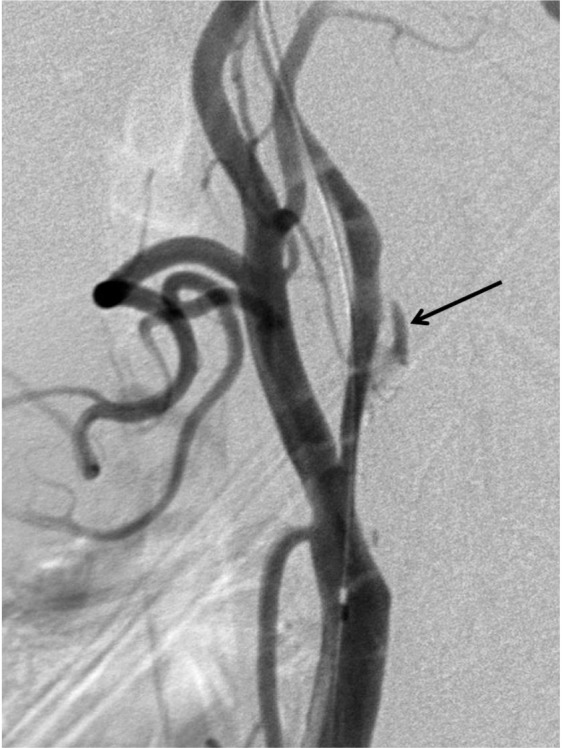
Fig. 2 Lateral view of post-angioplasty CCA angiogram shows development of dissection on the atheromatous plaque (arrow).

Fig. 3 After stent deployment, the left CCA angiogram AP view (A) shows significant very dense contrast accumulation (*) beyond the spindle shaped filling defect (arrows) captured in the EPD indicating significant slow flow beyond the filling defect. Subsequent intracranial AP view (B) showed slow filling of distal left ICA.

Fig. 4 10 minutes after Reopro® infusion, the forward flow through the filling defect shows re-established on the left CCA AP view.
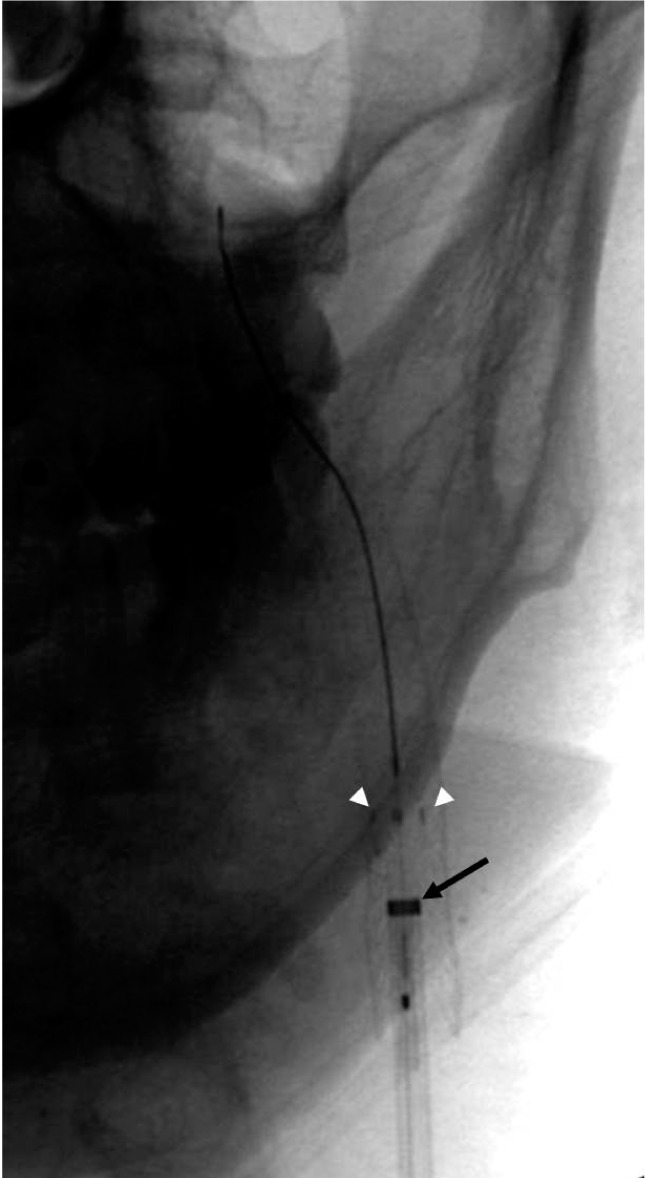
Fig. 5 AP spot film during the removal of the Rx-Accunet®, Rx-Accunet Retrieval device 2® and Shuttle® sheath. Note the 4 radio-opaque markers of the Rx-Accunet® are not completely opposed (white arrow heads) and the position of the Shuttle® sheath (arrow) which was advanced until the Rx-Accunet® wires can be straight enough not to be caught by the deployed stent struts.

Fig. 6 After the removal of the filling defect, AP view of extracranial (A) and intracranial (B) circulation on the left CCA angiogram show no additional filling defect.

Fig. 7 Gross picture (A) of the retrieved filling defect with EPD (removed from its delivery wire) shows spindle shaped 12 × 3 mm sized lesion. Calcium staining of the lesion (arrows) with underlying relative acelluar matrix (B) and Factor-VIII staining (C) for angiogenetic activity (arrows) indicating the lesion is a mature atheromatous plaque.
Reference
-
1. Angelini A, Reimers B, Barbera MD, Sacca S, Pasquetto G, Cernetti C, et al. Cerebral protection during carotid artery stenting: collection and histopathologic analysis of embolized debris. Stroke. 2002; 33:456–461. PMID: 11823652.2. Whitlow PL, Lylyk P, Londero H, Mendiz OA, Mathias K, Jaeger H, et al. Carotid artery stenting protected with an emboli containment system. Stroke. 2002; 33:1308–1314. PMID: 11988608.
Article3. Gray WA, Hopkins LN, Yadav S, Davis T, Wholey M, Atkinson R, et al. the ARCHeR Trial Collaborators. Protected carotid stenting in high-surgical-risk patients: the ARCHeR results. J Vasc Surg. 2006; 44:258–269. PMID: 16890850.
Article4. Hill MD, Morrish W, Soulez G, Nevelsteen A, Maleux G, Rogers C, et al. the MAVErIC International Investigators. Multicenter evaluation of a self-expanding carotid stent system with distal protection in the treatment of carotid stenosis. AJNR Am J Neuroradiol. 2006; 27:759–765. PMID: 16611760.5. Jansen O, Fiehler J, Hartmann M, Bruckmann H. Protection or nonprotection in carotid stent angioplasty: the influence of interventional techniques on outcome data from the SPACE trial. Stroke. 2009; 40:841–846. PMID: 19150863.6. Brown M, Rogers J, Bland J. Endovascular versus surgical treatment in patients with carotid stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a randomized trial. Lancet. 2001; 357:1729–1737. PMID: 11403808.7. Yadav J, Wholey M, Kuntz R, Fayad P, Katzen B, Mishkel G, et al. For the stenting and angioplasty with protection in patients at high risk for endarterectomy investigator. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004; 351:1493–1501. PMID: 15470212.8. Wholey Michael H, Al-Mubarak N, Wholey Mark H. Updated review of the global carotid artery stent registry. Catheter Cardiovasc Interv. 2003; 60:259–266. PMID: 14517936.9. Kastrup A, Groschel K, Krapf H, Brehm BR, Dichgans J, Schulz JB. Early outcome of carotid angioplasty and stenting with and without cerebral protection devices: a systematic review of the literature. Stroke. 2003; 34:813–819. PMID: 12624315.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Massive Cerebral Microemboli after Protected Carotid Artery Angioplasty and Stenting Using a Distal Filter Embolic Protection Device for a Vulnerable Plaque with a Lipid Rich Necrotic Core and Intraplaque Hemorrhage: A Case Report
- Novel use of a stent retriever as a distal filler protection device for prevention of secondary embolization
- The Use of Protection Device in Landmark-wire Technique of Symptomatic Subclavian Artery Occlusion with Combined Approach via Trans-femoral vs. Trans-brachial Arteries: Technical note
- Mobile Thrombus with an Ulcerative Plaque Diagnosed Using Ultrasonography in a Patient with Nonstenotic Carotid Artery Disease
- Stenting for Bilateral Renal Artery Occlusion with a Distal Embolic Protection Device
