Concurrent Diagnosis of Pulmonary Metastasis of Malignant Mixed Mullerian Tumor and Small Cell Lung Cancer
- Affiliations
-
- 1Division of Pulmonology, Department of Internal Medicine, Pusan Paik Hospital, Inje University College of Medicine, Busan, Korea. goodoc@gmail.com
- 2Department of Pathology, Pusan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- 3Department of Diagnostic Radiology, Pusan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- 4Department of Obstetrics and Gynecology, Pusan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 2050675
- DOI: http://doi.org/10.4046/trd.2012.73.1.56
Abstract
- A patient who has multiple lung masses with a history of malignancy in organs other than the lung is more likely to be diagnosed with metastatic rather than primary lung cancer. Rarely, metastatic cancer can coexist with primary. We experienced a case of concurrent diagnosis of primary small cell lung cancer and pulmonary metastasis of uterine malignant mixed Mullerian tumor (MMMT). The patient was a 52-year-old female with femur fracture and multiple lung masses with a history of an operation for uterine MMMT. The small cell lung cancer was diagnosed by bronchoscopic biopsy. The central lung mass decreased after chemotherapy for small cell lung cancer but multiple peripheral masses increased. A percutaneous biopsy for one of peripheral masses revealed metastatic uterine MMMT. We suggest that we have to consider the possible presence of concomitant malignancies of different origins in one organ especially with patients who had a history of malignancy in another organ.
MeSH Terms
Figure
-
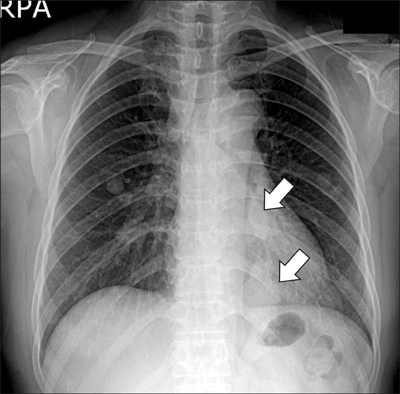
Figure 1 Initial chest X-ray. The chest radiography reveals two multilobulated masses (arrows) in retrocardiac area of the left lung and multiple round metastatic nodules in mid lung fields of both lung.
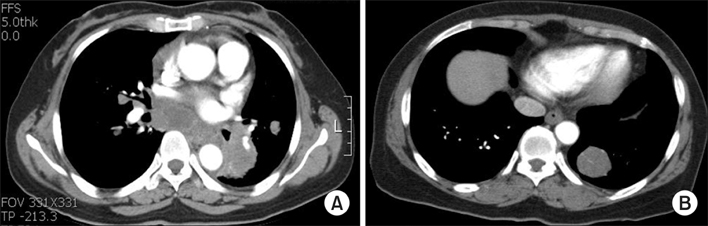
Figure 2 Initial chest computed tomography. (A) The axial image at the level of basal trunk of the left lower lobe bronchus reveals central lung cancer in the left lower lobe and massive subcarinal lymph node enlargement. (B) The axial image at the level of the lung base reveals a round metastatic mass in posterior basal segment of the left lower lobe.
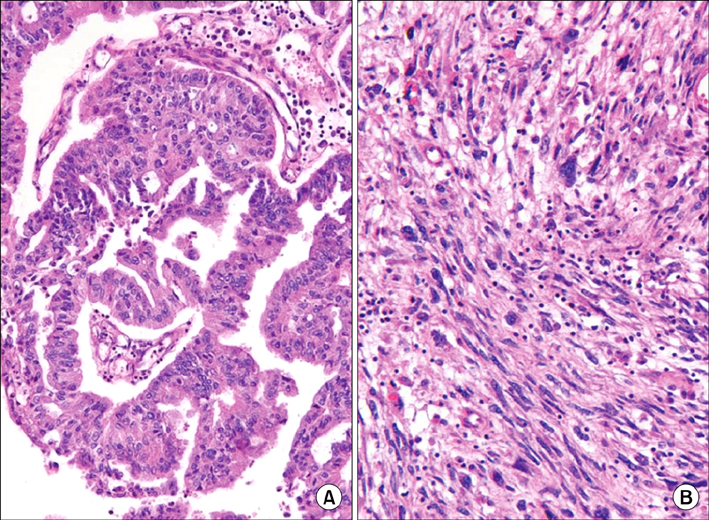
Figure 3 Histopathologic finding of uterus. Malignant mixed Müllerian tumor, also known as carcinosarcoma, is composed of malignant epithelial and stromal components. This figure reveals glandular epithelial (A) and sarcomatous (B) elements of uterus lesion (A, B, H&E stain, ×400).

Figure 4 The histopathologic finding of bronchoscopic biopsy tissue. This slide shows round to oval tumor cells which have minimal cytoplasm and are about twice as large as neutrophil. Their nucleus are 'salt and pepper' chromatin pattern and don't have a prominent nucleoli. We can also find frequent mitoses. These pathologic findings are consistent with small cell carcinoma (H&E stain, ×400).
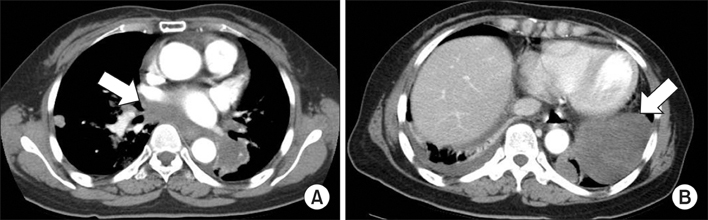
Figure 5 The computed tomography after two cycles of chemotherapy. (A) The mediastinal mass decreased (arrow). (B) The pleural based mass on left lower lobe increased markedly (arrow). Compare with pictures in Figure 2.
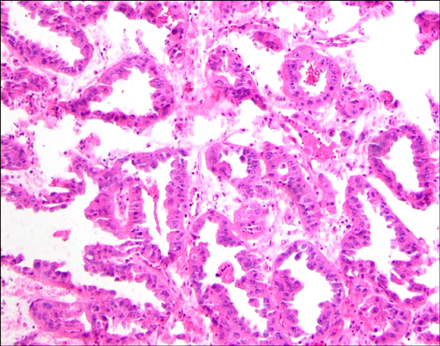
Figure 6 The histopathologic finding of femur bone. The bone lesion is composed of metastatic adenocarcinoma, which is similar to the carcinoma component of the uterus cancer. This is quite different from the lung lesion (H&E stain, decalcification, ×400).
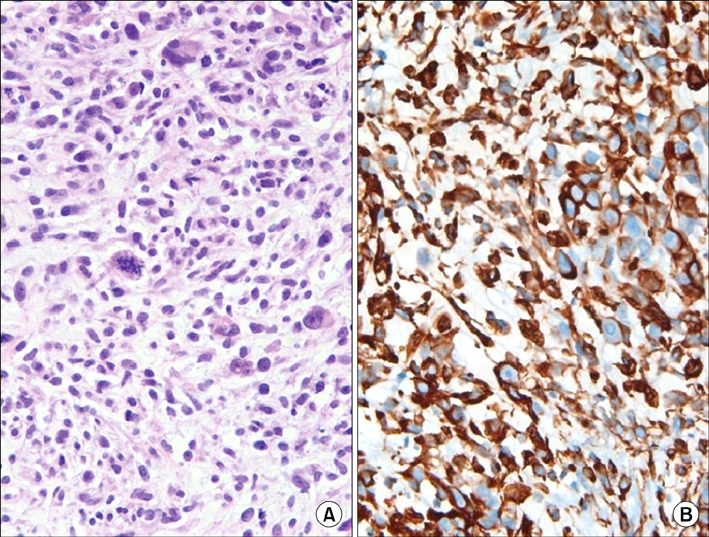
Figure 7 The histopathologic finding of percutaneous biopsy of peripheral lung mass. This slide reveals sarcoma which is composed of atypical spindle cells with frequent atypical mitoses. The pathologic features of uterine sarcoma elements resemble this (A). Vimentin immunohistochemistry was positve in this lung lesion (B) (A, H&E stain, ×400; B, vimentin immunohistochemistry, ×400).
Reference
-
1. Yonemori K, Kunitoh H, Sekine I. Small-cell lung cancer with lymphadenopathy in an 18-year-old female nonsmoker. Nat Clin Pract Oncol. 2006. 3:399–403.2. Peters WA 3rd, Bagley CM, Smith MR. CA-125: use as a tumor marker with mixed mesodermal tumors of the female genital tract. Cancer. 1986. 58:2625–2627.3. Barwick KW, LiVolsi VA. Malignant mixed mullerian tumors of the uterus: a clinicopathologic assessment of 34 cases. Am J Surg Pathol. 1979. 3:125–135.4. Gourley C, Al-Nafussi A, Abdulkader M, Smyth JF, Gabra H. Malignant mixed mesodermal tumours: biology and clinical aspects. Eur J Cancer. 2002. 38:1437–1446.5. Spanos WJ Jr, Peters LJ, Oswald MJ. Patterns of recurrence in malignant mixed müllerian tumor of the uterus. Cancer. 1986. 57:155–159.6. Bouros D, Papadakis K, Siafakas N, Fuller AF Jr. Patterns of pulmonary metastasis from uterine cancer. Oncology. 1996. 53:360–363.7. Ozkan M, Er O, Kaplan B, Altinbas M, Ozcelik B, Tokat F, et al. Presentation with superior vena cava syndrome secondary to solitary lung metastasis mimicking primary lung cancer following resection of a uterine malignant mixed mullerian tumor: brief case report. Eur J Obstet Gynecol Reprod Biol. 2005. 118:260–264.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Case of Malignant Mixed Mullerian Tumors
- Malignant Mixed Mullerian Tumor of the Fallopian Tube: Report of a Case
- A Case of Malignant Mixed Mullerian Tumor of the Uterus with Neuroendocrine Differentiation
- A case of Malignant Mixed Mullerian Tumor of the ovary
- Two Cases of Malignant Mixed Mullerian Tumor (MMMT) of the Ovary
