A Case of Pulmonary Paragonimiasis Mimicking Pulmonary Tuberculosis
- Affiliations
-
- 1Division of Pulmonology, Department of Internal Medicine, College of Medicine, Hanyang University, Seoul, Korea. drterry@hanyang.ac.kr
- KMID: 2050478
- DOI: http://doi.org/10.4046/trd.2007.63.5.440
Abstract
- Paragonimiasis mainly occurs by ingestion of raw or undercooked freshwater crabs or crayfish. In our country, the prevalence of paragonimiasis was high until late 1960s due to eating habits, but after the 1970s the prevalence of the disease has markedly decreased and now the disease is rarely seen. As the clinical and radiological features as well as the laboratory findings are similar to that of pulmonary tuberculosis, the differential diagnosis of pulmonary paragonimiasis is very difficult. We experienced a case of a patient with pulmonary paragonimiasis who was treated as having pulmonary tuberculosis.
Keyword
MeSH Terms
Figure
-
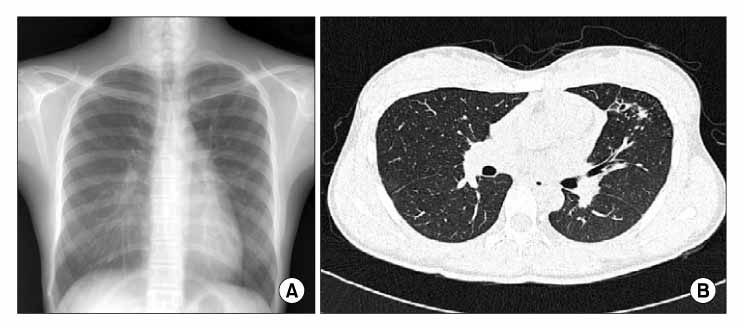
Figure 1 (A) On admission, chest radiography shows multiple nodular lesion at left upper lobe. (B) High resolution computed tomography of the chest shows cystic lesions and ground grass opacities at left upper lobe.
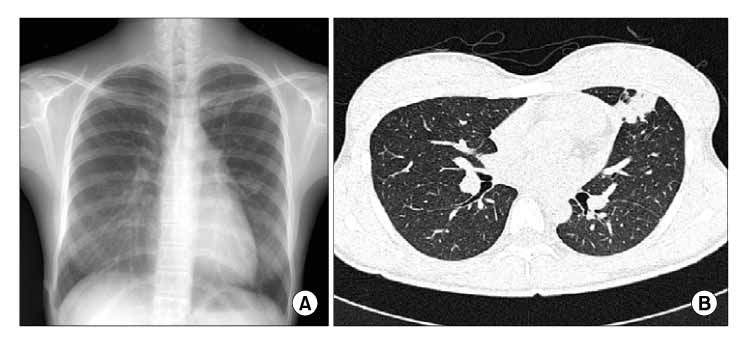
Figure 2 (A) 6 months after anti-TB medication. The chest radiography reveals aggravation of multiple nodues at left upper lobe. (B) High resolution computed tomography shows newly developed consolidation at left upper lobe.
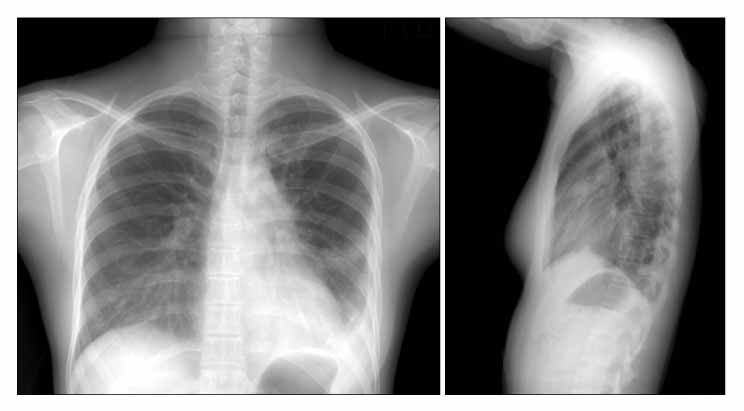
Figure 3 8 months after anti-TB medication. Chest PA and lateral radiography shows newly developed pleural effusion at left hemithorax.
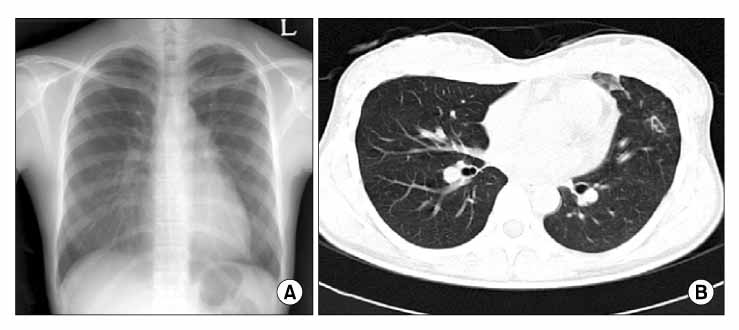
Figure 4 1 month after praziquantel medication for paragonimiasis. (A) Chest radiography shows improvement of nodular lesion at left upper lobe. (B) High resolution computed tomography shows improvement of cystic lesions and consolidation.
Reference
-
1. Sadun EH, Buck AA. Paragonimiasis in South Korea: immunodiagnostic, epidemiologic, clinical, roentgenologic and therapeutic studies. Am J Trop Med Hyg. 1960. 9:562–599.2. Choi DW. Paragonimus and paragonimiasis in Korea. Korean J Parasitol. 1990. 28s:79–102.3. Ministry of Health & Welfare. 7th national survey of the prevalence of intestinal parasitic infection in Korea. 2005. Gwacheon: Ministry of Health & Welfare.4. Jeon K, Koh WJ, Kim H, Kwon OJ, Kim TS, Lee KS, et al. Clinical feature of recently diagnosed pulmonary paragonimiasis in Korea. Chest. 2005. 128:1423–1430.5. Kuzucu A. Parasitic disease of the respiratory tract. Curr Opin Pulm Med. 2006. 12:212–221.6. Kim TS, Han J, Shim SS, Jeon K, Koh WJ, Lee I, et al. Pleuropulmonary paragonimiasis: CT findings in 31 patients. Am J Roentgenol. 2005. 185:616–621.7. Singh TN, Kananbala S, Devi KS. Pleuropulmonary paragonimiasis mimicking pulmonary tuberculosis: a report of three cases. Indian J Med Microbiol. 2005. 23:131–134.8. Shim YS, Cho SY, Han YC. Pulmonary paragonimiasis: a Korean perspective. Semin Respir Med. 1991. 12:35–45.9. Johnson JR, Falk A, Iber C, Davies S. Paragonimiasis in the United States: a report of nine cases in Hmong immigrants. Chest. 1982. 82:168–171.10. Singh TS, Mutum SS, Razaque MA. Pulmonary paragonimiasis: clinical features, diagnosis and treatment of 39 cases in Manipur. Trans R Soc Trop Med Hyg. 1986. 80:967–971.11. Cho SY, Lee DK, Kang SY, Kim SI. An epidemiological study of human paragonimiasis by means of micro-ELISA. Korean J Parasitol. 1983. 21:246–256.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Pulmonary Paragonimiasis Mimicking Lung Cancer Diagnosed by EBUS-TBNA
- Identification of pulmonary paragonimiasis using Ziehl-Neelsen stain
- Pulmonary paragonimiasis: CT findings
- Clinical Study of Pulmonary Paragonimiasis
- A Case of Pulmonary Paragonimiasis Presented as Solitary Pulmonary Nodule and Suspected as Lung Cancer on (18)F-Fluorodeoxyglucose Positron Emission Tomography
