Clin Endosc.
2014 Mar;47(2):188-191. 10.5946/ce.2014.47.2.188.
An Unusual Case of Duodenal Perforation Caused by a Lollipop Stick: A Case Report
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea. p1052ccy@hanmail.net
- KMID: 2049008
- DOI: http://doi.org/10.5946/ce.2014.47.2.188
Abstract
- Most ingested foreign bodies often pass through the gastrointestinal tract uneventfully; however, complications such as perforation do occur. Most cases of perforation are caused by thin, pointed objects such as needles, toothpicks, or fish and chicken bones. Herein, we report an unusual case of duodenal perforation caused by a lollipop stick with blunt ends. A 23-year-old woman was admitted to the emergency department complaining of epigastric and right upper quadrant pain for the last 2 days. Abdominal computed tomography scans confirmed the presence of a foreign body in the duodenum, with signs of duodenal perforation and inflammation. The patient was not aware of ingesting the foreign body. Endoscopy revealed the presence of a lollipop stick in the duodenum, which was removed with forceps. The duodenal perforation was successfully managed by using hemoclips and a detachable snare.
Keyword
MeSH Terms
Figure
-
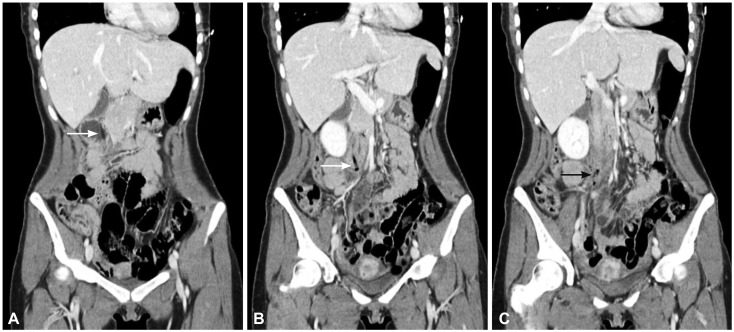
Fig. 1 (A-C) Computed tomography findings. A stick-like foreign body was observed in the duodenum (white arrow). Mottled air density was observed around the third portion of the duodenum (black arrow).
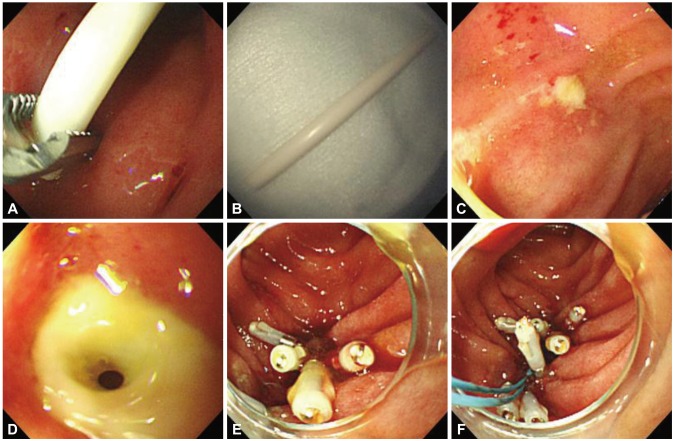
Fig. 2 Endoscopic findings. (A, B) A lollipop stick was removed by using rat-tooth forceps. (C) A proximal small ulcer with exudates was observed in the third portion of the duodenum. (D) A distal ulcer with air bubble was observed in the third portion of the duodenum. (E) Five hemoclips were applied to the margin of the duodenal perforation. (F) A detachable snare was used to approximate the ends of the perforation.
Reference
-
1. Velitchkov NG, Grigorov GI, Losanoff JE, Kjossev KT. Ingested foreign bodies of the gastrointestinal tract: retrospective analysis of 542 cases. World J Surg. 1996; 20:1001–1005. PMID: 8798356.
Article2. Goh BK, Chow PK, Quah HM, et al. Perforation of the gastrointestinal tract secondary to ingestion of foreign bodies. World J Surg. 2006; 30:372–377. PMID: 16479337.
Article3. Coulier B, Tancredi MH, Ramboux A. Spiral CT and multidetectorrow CT diagnosis of perforation of the small intestine caused by ingested foreign bodies. Eur Radiol. 2004; 14:1918–1925. PMID: 15378256.
Article4. Chiu YH, Hou SK, Chen SC, et al. Diagnosis and endoscopic management of upper gastrointestinal foreign bodies. Am J Med Sci. 2012; 343:192–195. PMID: 21804366.
Article5. Cheng W, Tam PK. Foreign-body ingestion in children: experience with 1,265 cases. J Pediatr Surg. 1999; 34:1472–1476. PMID: 10549750.
Article6. Marom T, Goldfarb A, Russo E, Roth Y. Battery ingestion in children. Int J Pediatr Otorhinolaryngol. 2010; 74:849–854. PMID: 20538351.
Article7. Ambe P, Weber SA, Schauer M, Knoefel WT. Swallowed foreign bodies in adults. Dtsch Arztebl Int. 2012; 109:869–875. PMID: 23293675.
Article8. Smith MT, Wong RK. Foreign bodies. Gastrointest Endosc Clin N Am. 2007; 17:361–382. PMID: 17556153.
Article9. ASGE Standards of Practice Committee. Ikenberry SO, Jue TL, et al. Management of ingested foreign bodies and food impactions. Gastrointest Endosc. 2011; 73:1085–1091. PMID: 21628009.
Article10. Webb WA. Management of foreign bodies of the upper gastrointestinal tract: update. Gastrointest Endosc. 1995; 41:39–51. PMID: 7698623.
Article11. Ragazzi M, Delcò F, Rodoni-Cassis P, Brenna M, Lavanchy L, Bianchetti MG. Toothpick ingestion causing duodenal perforation. Pediatr Emerg Care. 2010; 26:506–507. PMID: 20622631.
Article12. Binmoeller KF, Grimm H, Soehendra N. Endoscopic closure of a perforation using metallic clips after snare excision of a gastric leiomyoma. Gastrointest Endosc. 1993; 39:172–174. PMID: 8495838.
Article13. Hachisu T. A new detachable snare for hemostasis in the removal of large polyps or other elevated lesions. Surg Endosc. 1991; 5:70–74. PMID: 1948617.
Article14. Leem JM, Han JH, Ko BS, et al. A case of fishbone-induced esophageal perforation closed by endoscopic clipping. Korean J Gastrointest Endosc. 2010; 41:151–154.15. Han WS, Park JJ, Lee BJ, et al. A case of foreign body induced esophageal perforation repaired by endoscopic clipping. Korean J Gastrointest Endosc. 2007; 35:28–32.16. Jones WG 2nd, Ginsberg RJ. Esophageal perforation: a continuing challenge. Ann Thorac Surg. 1992; 53:534–543. PMID: 1489367.
Article17. Kaneko T, Akamatsu T, Shimodaira K, et al. Nonsurgical treatment of duodenal perforation by endoscopic repair using a clipping device. Gastrointest Endosc. 1999; 50:410–413. PMID: 10462667.
Article18. Boškoski I, Tringali A, Landi R, et al. Endoscopic retrieval of a duodenal perforating teaspoon. World J Gastrointest Endosc. 2013; 5:186–188. PMID: 23596543.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An unusual cause of duodenal perforation due to a lollipop stick
- Perforated Duodenal Diverticulum Caused by Bezoar: A Case Report
- Conservative Management of a Duodenal Perforation after Trauma
- Duodenal Perforation due to Hemoclipping for the Dieulafoy's Lesion in a Duodenal Diverticulum
- Unexpectedly Discovered Duodenal Perforation
