Huge Liposarcoma of Esophagus Resected by Endoscopic Submucosal Dissection: Case Report with Video
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Gachon University Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea. junwonchung@hanmail.net
- 2Department of Pathology, Gachon University Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea.
- KMID: 2048938
- DOI: http://doi.org/10.5946/ce.2013.46.3.297
Abstract
- Liposarcoma is one of the most common soft tissue sarcomas occurring in adults, but it rarely occurs in the gastrointestinal tract and more uncommonly in the esophagus. To the best of our knowledge, there are only 19 reported cases of esophageal liposarcoma in the literature published in English language up to the year 2008, and they were all treated by surgical methods. Here, we report a case of primary liposarcoma of the esophagus which was treated with endoscopic submucosal dissection (ESD). ESD was well tolerated in this patient, suggesting that it may be a therapeutic option for primary esophageal sarcomas.
Keyword
MeSH Terms
Figure
-
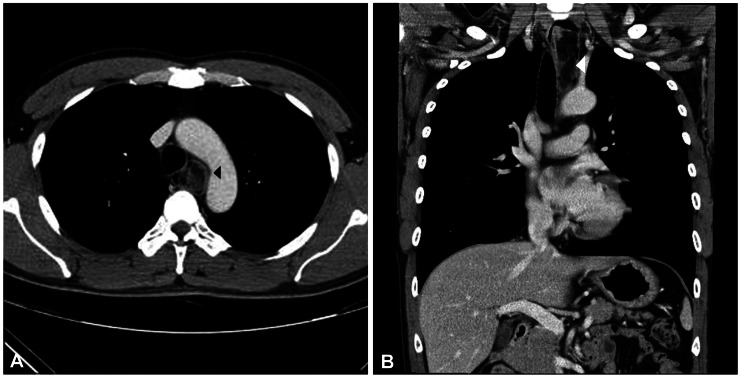
Fig. 1 Contrast-enhanced computed tomography scan (A, transverse view; B, coronal view) images demonstrate a tumor (arrowheads) protruding into the esophageal lumen. The large tumor is almost completely obstructing the esophagus.
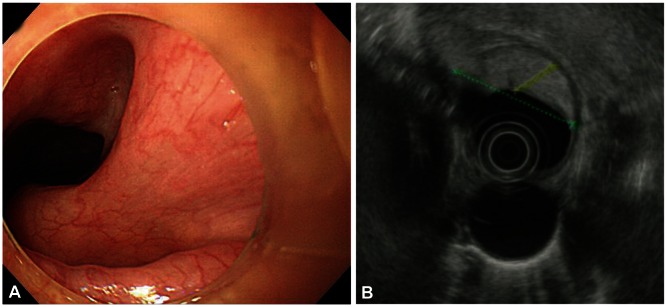
Fig. 2 (A) Esophagogastroduodenoscopy image shows a huge mass with stalk. (B) Endoscopic ultrasonography image shows a submucosal mass located in the posterior wall of upper to mid esophagus. The diameters of the mass were 12.7 and 37.1 mm, respectively.
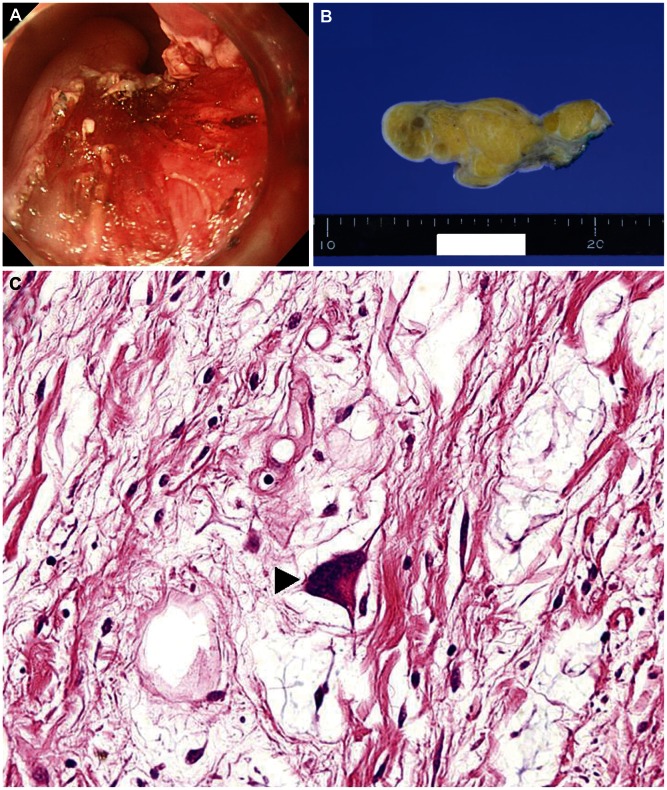
Fig. 3 (A) Esophagogastroduodenoscopy image during endoscopic submucosal dissection. (B) Gross image shows a yellowish, multilobulating mass divided by fibrous septa. (C) Microscopic finding shows a bizarre, big nucleus (arrowhead) suggesting liposarcoma rather than lipoma (H&E stain, ×200).
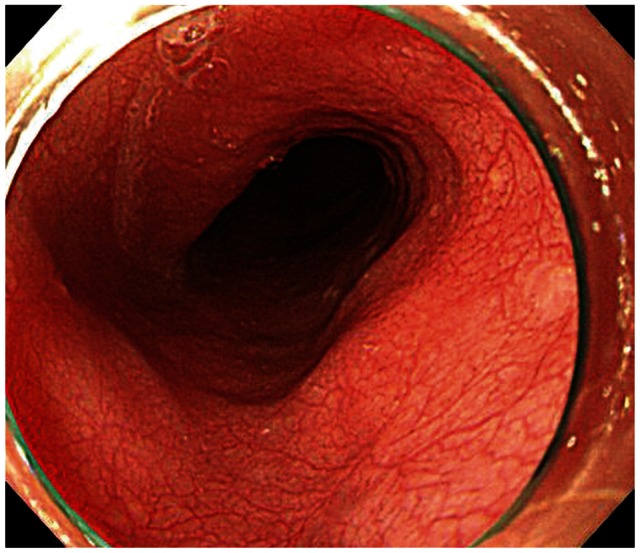
Fig. 4 On esophagogastroduodenoscopy after endoscopic submucosal dissection, there is no evidence of recurrence or metastasis.
Reference
-
1. Garcia M, Buitrago E, Bejarano PA, Casillas J. Large esophageal liposarcoma: a case report and review of the literature. Arch Pathol Lab Med. 2004; 128:922–925. PMID: 15270604.
Article2. Yang B, Shi PZ, Li X, Xu RJ. Well-differentiated liposarcoma of esophagus. Chin Med J (Engl). 2006; 119:438–440. PMID: 16542592.
Article3. Białek A, Wiechowska-Kozłowska A, Pertkiewicz J, et al. Endoscopic submucosal dissection for treatment of gastric subepithelial tumors (with video). Gastrointest Endosc. 2012; 75:276–286. PMID: 22032850.4. Shi Q, Zhong YS, Yao LQ, Zhou PH, Xu MD, Wang P. Endoscopic submucosal dissection for treatment of esophageal submucosal tumors originating from the muscularis propria layer. Gastrointest Endosc. 2011; 74:1194–1200. PMID: 21963065.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effective Endoscopic Submucosal Dissection of a Huge Esophageal Liposarcoma: A Case Report
- A Case of Endoscopic Submucosal Dissection for Esophageal Adenocarcinoma Arising from Ultrashort-Segment Barrett's Esophagus
- A Case of Recurrence after Endoscopic Submucosal Dissection of Esophageal Adenocarcinoma Arising from Barrett's Esophagus
- Pedunculated liposarcoma of esophagus: a case report
- Pyloric Gland Adenoma of the Esophagus Treated by Endoscopic Submucosal Dissection: A Case Report
