Infect Chemother.
2012 Aug;44(4):310-314. 10.3947/ic.2012.44.4.310.
A Case of Native Valve Infective Endocarditis Caused by Bacillus cereus
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. shhan74@yuhs.ac
- 2AIDS Research Institute, Yonsei University College of Medicine, Seoul, Korea.
- 3Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 4Department of Laboratory Medicine and Research Institute of Bacterial Resistance, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2045553
- DOI: http://doi.org/10.3947/ic.2012.44.4.310
Abstract
- Bacillus cereus is a ubiquitous organism that often contaminates microbiological cultures but rarely causes serious infections in humans. It is the causative organism of infective endocarditis (IE), a disease typically associated with intravenous (IV) drug abusers. Thus, almost all reported cases have involved the tricuspid valve. We report a case of native mitral valve (MV) IE caused by B. cereus in a 54 year-old man with moderate MV regurgitation but no apparent history of IV drug use. He presented with fever and dyspnea on exertion, symptoms which had been ongoing for 2 months. B. cereus infection was determined by blood culture examination. A transthoracic echocardiography revealed that mobile vegetations had attached to the MV. He was treated with IV antibiotics for a total of 6 weeks and received MV replacement surgery. He has maintained a good clinical recovery without complications since discharge.
Keyword
MeSH Terms
Figure
-
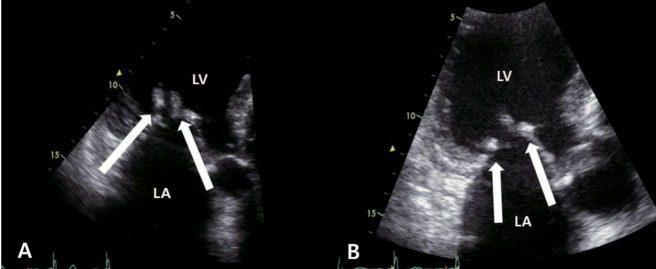
Figure 1 Transthoracic echocardiography in the parasternal long axis view as observed upon admission (A) and on the 12th hospital day (B) which reveal two vegetations of 1.3×0.6 cm and 1.2×0.7 cm size attached on the anterior and posterior of the mitral valve leaflet, respectively. LA, left atrium; LV, left ventricle.
Reference
-
1. Murdoch DR, Corey GR, Hoen B, Miró JM, Fowler VG Jr, Bayer AS, Karchmer AW, Olaison L, Pappas PA, Moreillon P, Chambers ST, Chu VH, Falcó V, Holland DJ, Jones P, Klein JL, Raymond NJ, Read KM, Tripodi MF, Utili R, Wang A, Woods CW, Cabell CH. International Collaboration on Endocarditis-Prospective Cohort Study (ICE-PCS) Investigators. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Arch Intern Med. 2009. 169:463–473.
Article2. Shin SY, Park YS, Choi JY, Cho CH, Park YS, Kim CO, Yoon HJ, Kim HY, Yum JS, Lee KS, Choi YH, Huh AJ, Hong SK, Song YG, Kim JM. Changing trends of infective endocarditis according to the change in health care system in Korea. Korean J Med. 2005. 68:157–167.3. Son JS, Ki HK, Oh WS, Peck KR, Lee NY, Park KH, Park PW, Song JH. Observation of clinical characteristics of infective endocarditis. Infect Chemother. 2005. 37:152–160.4. Castedo E, Castro A, Martin P, Roda J, Montero CG. Bacillus cereus prosthetic valve endocarditis. Ann Thorac Surg. 1999. 68:2351–2352.
Article5. Thomas BS, Bankowski MJ, Lau WK. Native valve Bacillus cereus endocarditis in a non-intravenous-drug-abusing patient. J Clin Microbiol. 2012. 50:519–521.
Article6. Tuazon CU, Murray HW, Levy C, Solny MN, Curtin JA, Sheagren JN. Serious infections from Bacillus sp. JAMA. 1979. 241:1137–1140.
Article7. Sliman R, Rehm S, Shlaes DM. Serious infections caused by Bacillus species. Medicine (Baltimore). 1987. 66:218–223.
Article8. Drobniewski FA. Bacillus cereus and related species. Clin Microbiol Rev. 1993. 6:324–338.
Article9. Abusin S, Bhimaraj A, Khadra S. Bacillus Cereus Endocarditis in a permanent pacemaker: a case report. Cases J. 2008. 1:95.10. Cone LA, Dreisbach L, Potts BE, Comess BE, Burleigh WA. Fatal Bacillus cereus endocarditis masquerading as an anthrax-like infection in a patient with acute lymphoblastic leukemia: case report. J Heart Valve Dis. 2005. 14:37–39.11. Martín Cadenas P, Sánchez Alor G, Aguilar Ruiz JC, Castedo E, Daza R, Mendaza P. Endocarditis by Bacillus cereus 1 in prosthetic mitral valve. Enferm Infecc Microbiol Clin. 1998. 16:102–104.12. Yamamura M, Aoki K, Takanashi S, Tadokoro M, Furuta S, Mizokami T. A case of Bacillus cereus prosthetic valve endocarditis. Kyobu Geka. 1994. 47:232–234.13. Steen MK, Bruno-Murtha LA, Chaux G, Lazar H, Bernard S, Sulis C. Bacillus cereus endocarditis: report of a case and review. Clin Infect Dis. 1992. 14:945–946.
Article14. Weller PF, Nicholson A, Braslow N. The spectrum of Bacillus bacteremias in heroin addicts. Arch Intern Med. 1979. 139:293–294.
Article15. Wanvarie S, Rochanawatanon M. Bacillus cereus endocarditis. J Med Assoc Thai. 1979. 62:34–38.16. Block CS, Levy ML, Fritz VU. Bacillus cereus endocarditis. A case report. S Afr Med J. 1978. 53:556–557.17. Craig CP, Lee WS, Ho M. Letter: Bacillus cereus endocarditis in an addict. Ann Intern Med. 1974. 80:418–419.18. Oster HA, Kong TQ. Bacillus cereus endocarditis involving a prosthetic valve. South Med J. 1982. 75:508–509.19. Park SH, Yang JM, Jeong HR, Lee MY, Seoung KB, Chae JS, Choi KB, Chong YS. A case of infective endocarditis caused by Bacillus species. Korean J Intern Med. 1990. 38:131–136.20. Luna VA, King DS, Gulledge J, Cannons AC, Amuso PT, Cattani J. Susceptibility of Bacillus anthracis, Bacillus cereus, Bacillus mycoides, Bacillus pseudomycoides and Bacillus thuringiensis to 24 antimicrobials using Sensititre automated microbroth dilution and Etest agar gradient diffusion methods. J Antimicrob Chemother. 2007. 60:555–567.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of native valve infective endocarditis caused by Microbacterium species
- A case of Haemophilus aphrophilus native valve endocarditis
- A Case of Infective Endocarditis caused by Abiotrophia defectiva in Korea
- A Case of Bacillus Cereus Infection with Pneumonia and Bactermia
- A Case of Native Valve Infective Endocarditis Caused by Staphylococcus lugdunensis
