Parosteal Lipoma in the Metatarsus: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Korea. superdrsys@hotmail.com
- 2Department of Pathology, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Korea.
- KMID: 2045019
- DOI: http://doi.org/10.14193/jkfas.2015.19.3.132
Abstract
- We experienced a rare case of parosteal lipoma, which located on the periosteum of the foot 4th metatarsus. A 22-year-old woman visited the hospital with painful mass in her foot. Based on the assessment of plain radiographs, computed tomography scan, and magnetic resonance image, it was suspected as lipoma. Marginal excision was performed and parosteal lipoma was confirmed histologically. Any local recurrence and complications were not observed in 2 years after surgery.
Keyword
Figure
-

Figure 1. Preoperative photographs showed a focal, ovalshaped protrusion in the dorsal surface of 4th metatarsal base. (A) Anteroposterior view. (B) Lateral view.

Figure 2. Preoperative plain radiographs showed an ovalshaped radiolucent lesion around 4th metatarsal base. (A) Anteroposterior view. (B) Oblique view.
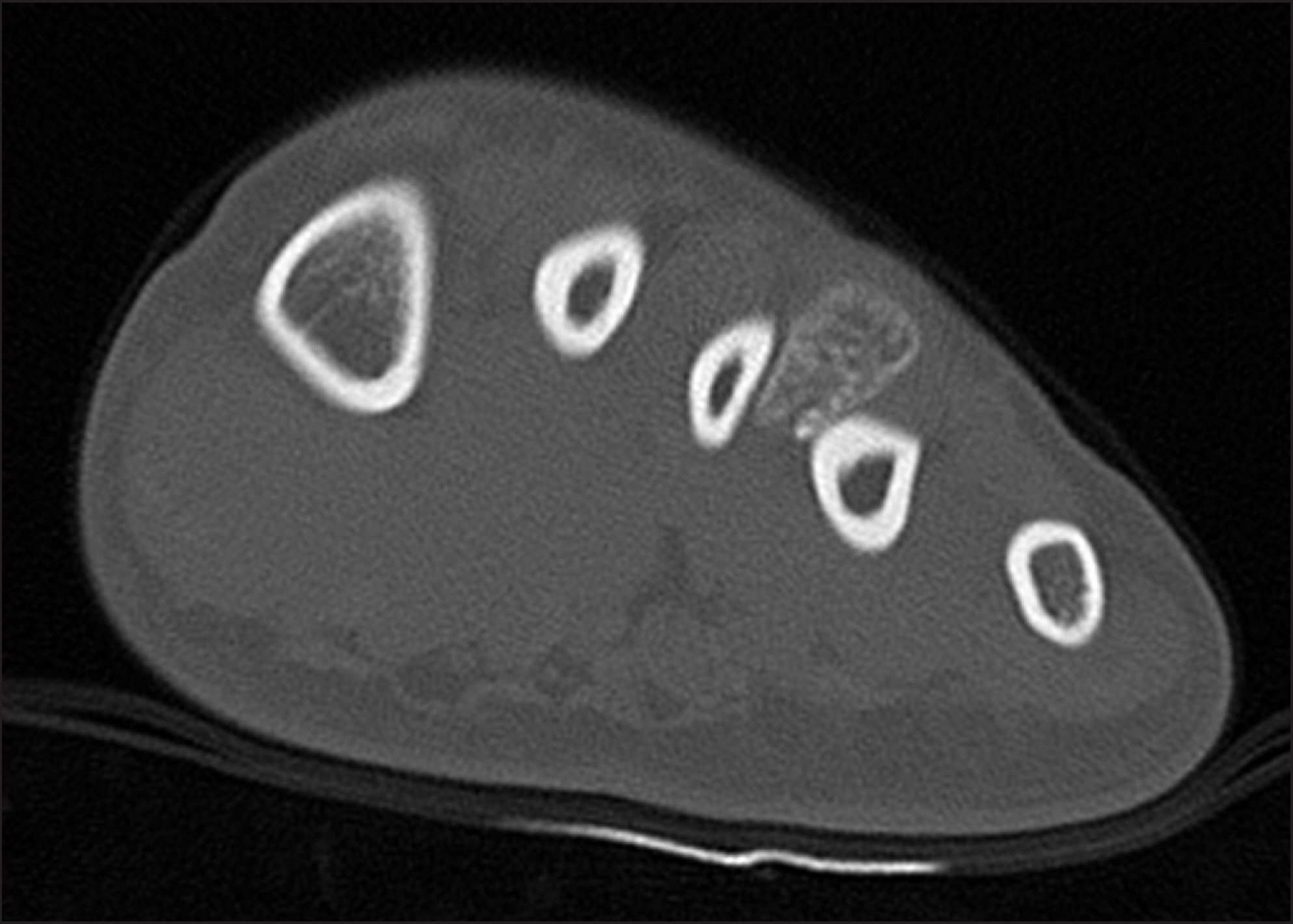
Figure 3. Preoperative computed tomography scan showed that the mass did not communicate with the adjacent bone and had cortical irregularity and hyperostosis at 4th metatarsal base.
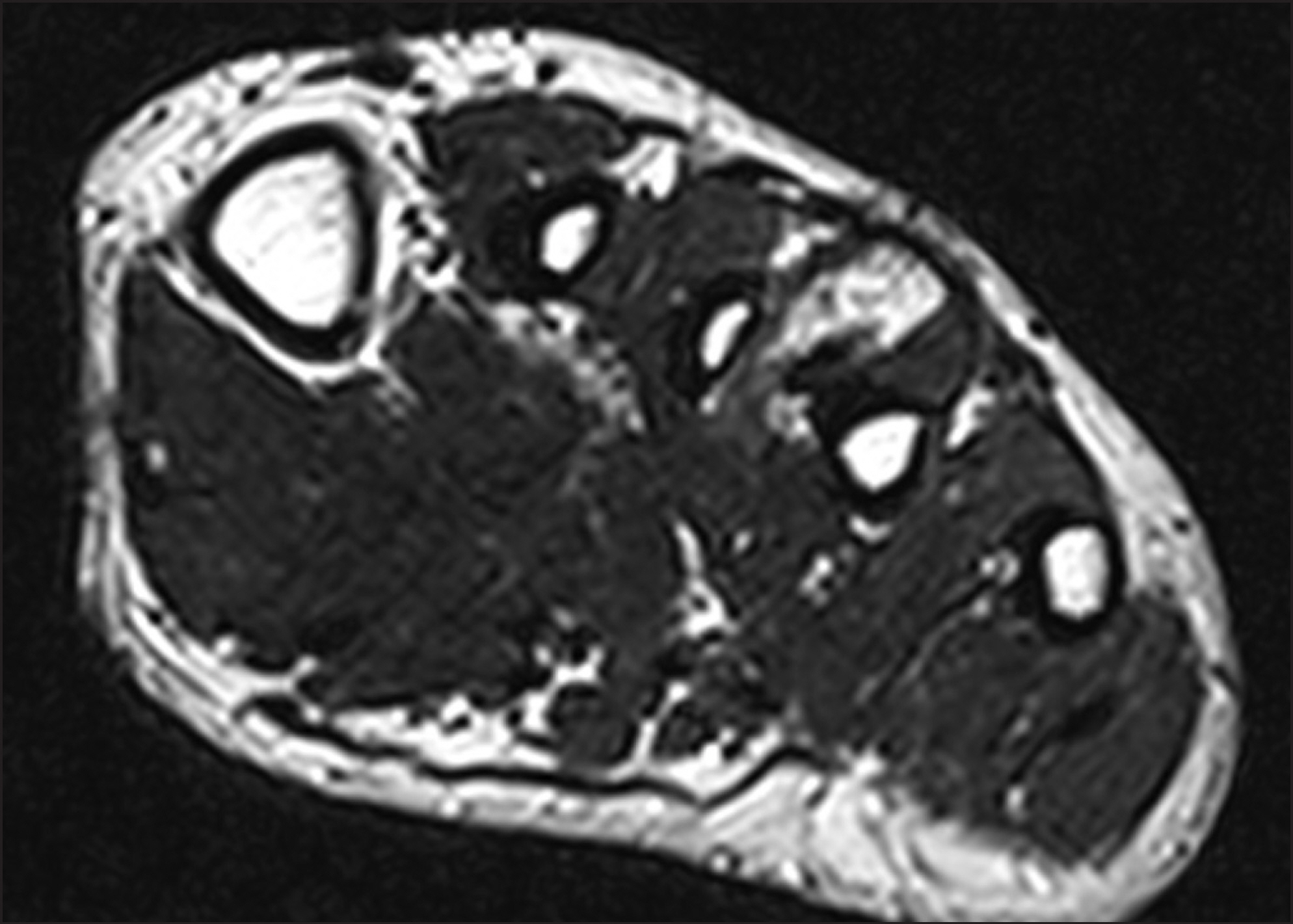
Figure 4. Preoperative axial T2-weighted magnetic resonance image showed ossified mass with high signal intensity.
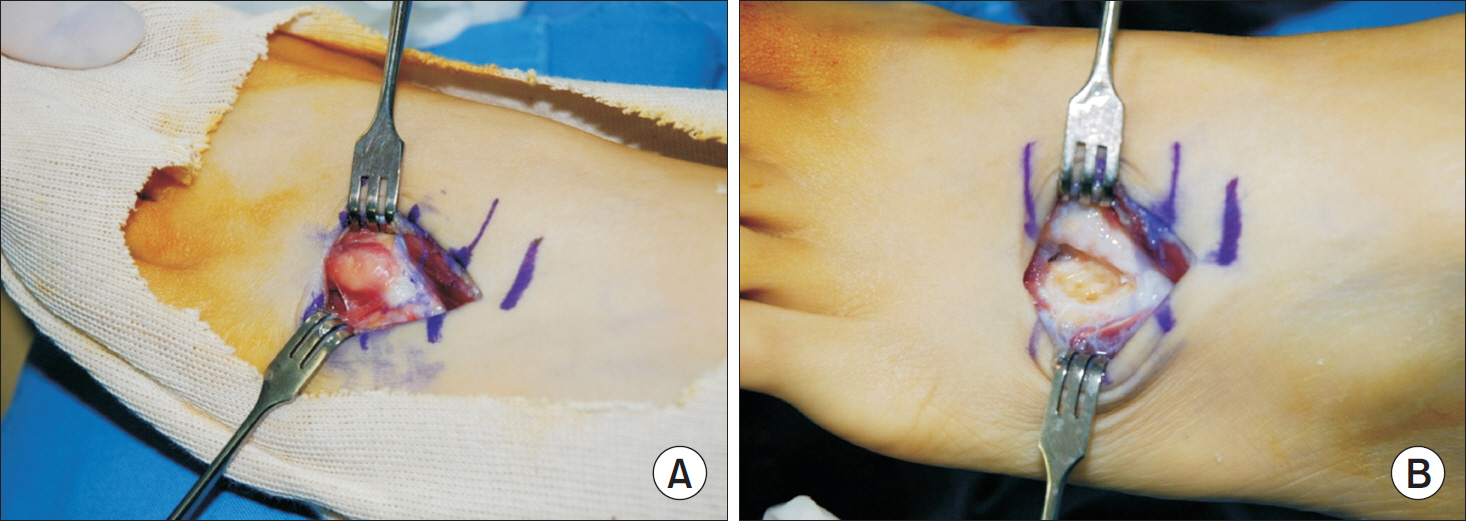
Figure 5. (A) Intraoperative photograph showed oval shaped mass attached to 4th metatarsus. (B) The cortical bone of the metatarsus was intact after excision of mass.
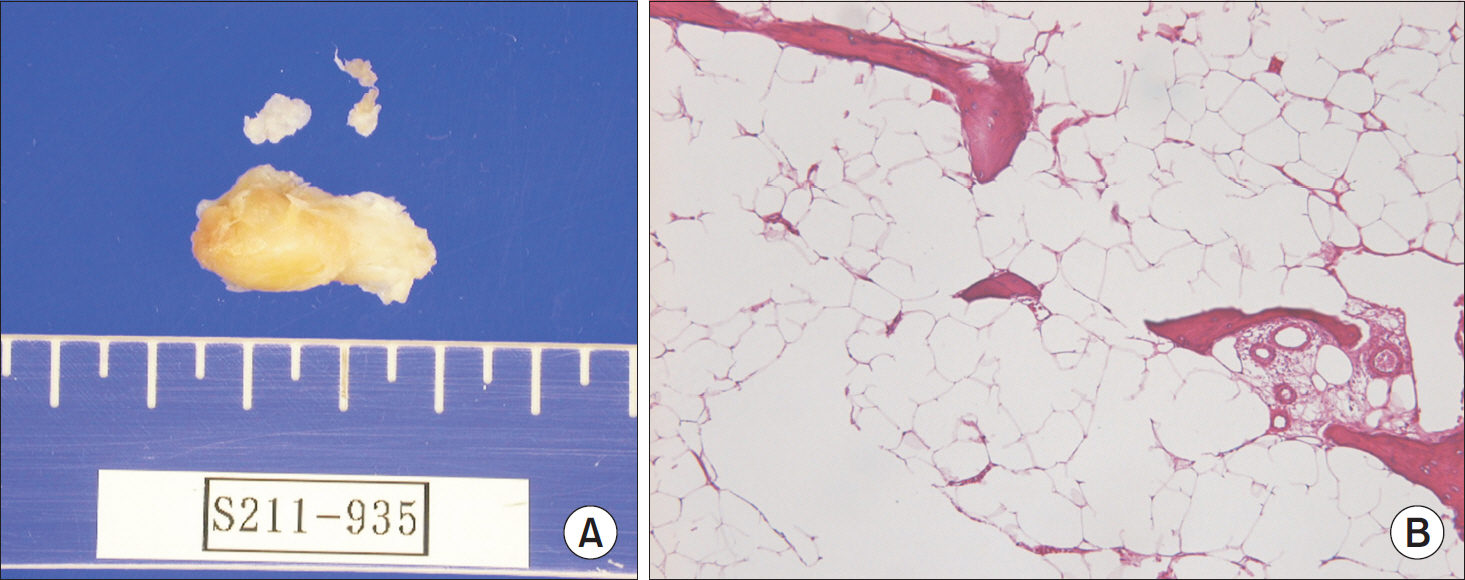
Figure 6. (A) After marginal excision, 2.4 ×1.0×1.0 cm sized mass was excised including the periosteum. (B) Microscopically, the mass was mainly composed of mature lipocytes (H&E stain, ×100).

Figure 7. Postoperative plain radiographs at 2 years showed no recurrence. (A) Anteroposterior view. (B) Oblique view.
Reference
-
References
1. Fleming RJ, Alpert M, Garcia A. Parosteal lipoma. Am J Roentgenol. 1962; 87:1075–84.2. Rhee SK, Lee HS, Chung JW, Jheong HK. Parosteal lipoma with hyperostosis: two cases report. J Korean Bone Joint Tumor Soc. 2001; 7:105–9.3. Kim DY, Jeon HS, Jeon SJ, Noh HK, Kang SG, Song JU, et al. Parosteal lipoma of the femur with hyperostosis: a case report1 J Korean Bone Joint Tumor Soc. 2012; 18:104–8.4. Kwon BC, Lee BT, Park SW, Rhee NK, Choi SJ, Jun SY. Compressive neuropathy of posterior interosseous nerve caused by parosteallipoma of the proximal radius. J Korean Soc Surg Hand. 2007; 12:84–71.5. Kim JY, Jung SL, Park YH, Park SH, Kang YK. Parosteal lipoma with hyperostosis. Eur Radiol. 1999; 9:1810–2.6. Goldman AB, DiCarlo EF, Marcove RC. Case report 7741 Coincidental parosteal lipoma with osseous excresence and intramuscular lipoma. Skeletal Radiol. 1993; 22:138–45.7. Greco M, Mazzocchi M, Ribuffo D, Dessy LA, Scuderi N. Parosteal lipoma. Report of 15 new cases and a review of the literature. Ann Ital Chir. 2013; 84:229–351. 81 Krajewska I, Vernon-Roberts B, Sorby-Adams G. Parosteal (periosteal) lipoma1 Pathology1 1988;20: 179–83.9. Murphey MD, Johnson DL, Bhatia PS, Neff JR, Rosenthal HG, Walker CW. Parosteal lipoma: MR imaging characteristics. Am J Roentgenol. 1994; 162:105–10.
Article10. Avram R, Hynes NM. Posterior interosseous nerve compression secondary to a parosteal lipoma: case report and literature review. Can J Plast Surg1. 2004; 12:69–72.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Parosteal Lipoma Associated with a Growing Osteochondroma of the Right Ilium
- Parosteal Lipoma of the Tibia: A Case Report
- Parosteal Lipoma Associated with Underlying Recurrent Bizarre Parosteal Osteochondromatous Proliferation (Nora's Lesion) of the Hand
- Parosteal Chondrolipoma of the Scapula: A Case Report
- Parosteal Lipoma of the Femur with Hyperostosis: A Case Report
