Relationships Between Canal Occlusion and Neurologic Deficits, and Between Kyphotic Deformities and Fracture Types in Unstable Thoracolumbar Burst Fractures
- Affiliations
-
- 1Department of Orthopedic Surgery, Bundang Cha Hospital, College of Medicine, Pochon Cha University, Sung-Nam, Korea. shinde@cha.ac.kr
- KMID: 2040779
- DOI: http://doi.org/10.4184/jkss.2006.13.1.40
Abstract
-
STUDY DESIGN: A retrospective study.
OBJECTIVES
To evaluate the relationships between spinal canal occlusion and neurologic deficits, and between spinal canal decompression and neurologic recovery in thoracolumbar burst fractures. Kyphotic deformities, based on the fracture types in short-segment instrumentation and fusion, were evaluated to determine effective operative methods. SUMMARY OF LITERATURE REVIEW: In thoracolumbar burst fractures, the relationship between spinal canal occlusion and neurologic deficits remains controversial; and definitive guidelines for short-segment instrumentation and fusion have not been established .
MATERIALS AND METHODS
Surgically treated thoracolumbar burst fractures (N=112) were analyzed retrospectively. Spinal canal occlusion in both neurologically intact and deficient groups, and neurologic recovery as a result of spinal canal decompression, were evaluated based on Frankel's grades. Kyphotic deformities based on the Denis classification and McCormack's load sharing classification were evaluated in 86 short-segment instrumentation patients.
RESULTS
Spinal canal occlusion in the neurologically deficient group (51.8%) was significantly higher than that in the neurologically intact group (31.4%) (p < 0.05). Although 29 patients who recovered neurologically and 25 who did not, demonstrated 20.4% and 19.5% of spinal canal decompression, respectively, it was not significant (p > 0.05). Kyphotic deformities were increased significantly in Denis type A, B and groups with more than 7 points in the load sharing classification (p < 0.05).
CONCLUSION
In thoracolumbar burst fractures, the degree of initial spinal canal occlusion was more significantly related with neurologic deficits than with postoperative spinal canal decompression. Extended instrumentation and fusion is recommended for reducing postoperative kyphotic deformities in Denis type A, B and groups with more than 7 points in the load sharing classification.
MeSH Terms
Figure
-
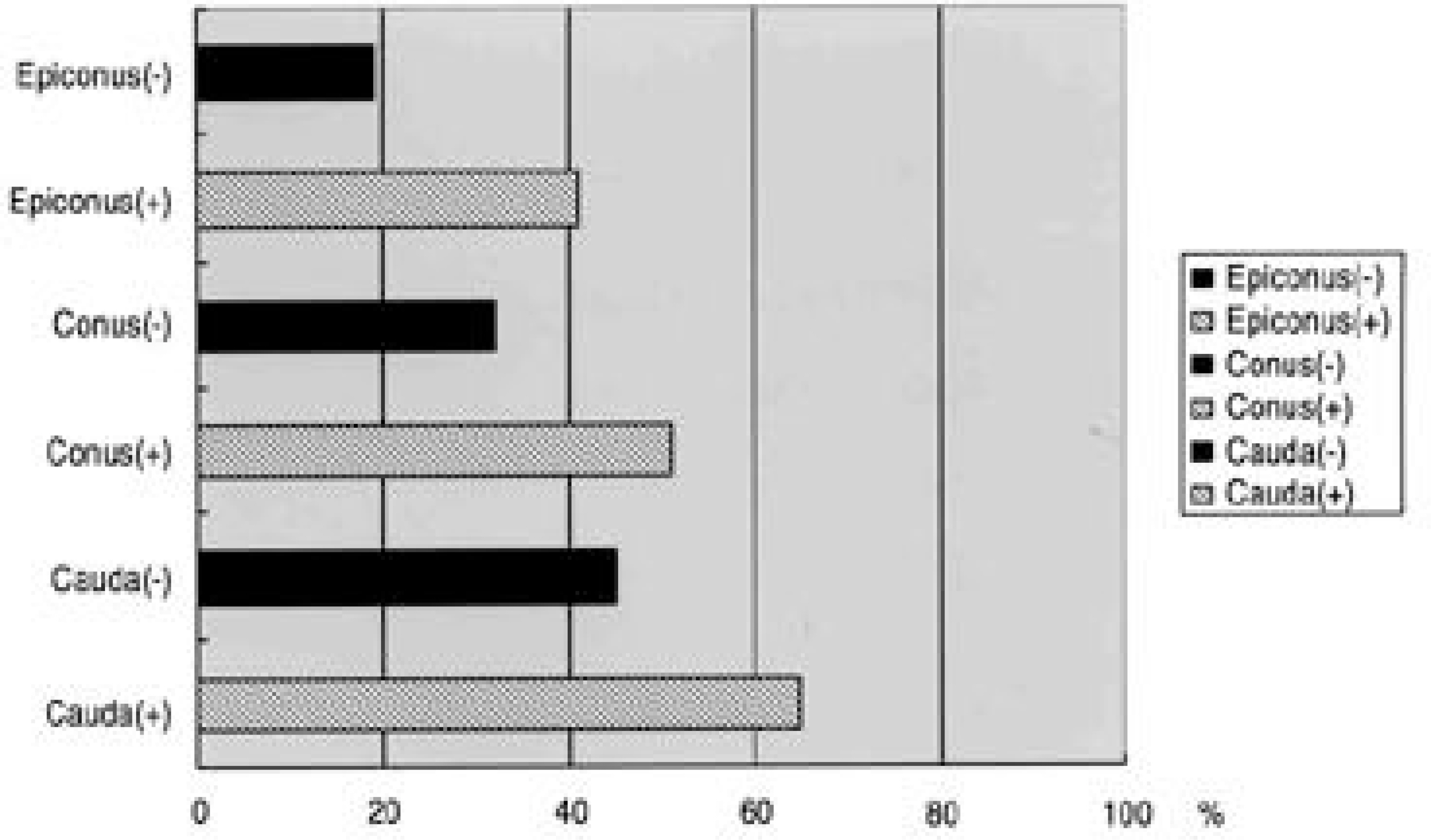
Fig. 1. Canal occlusion of neurologic intact group and neurologic deficit group. (-): neurologic intact group, (+): neurologic deficit group.
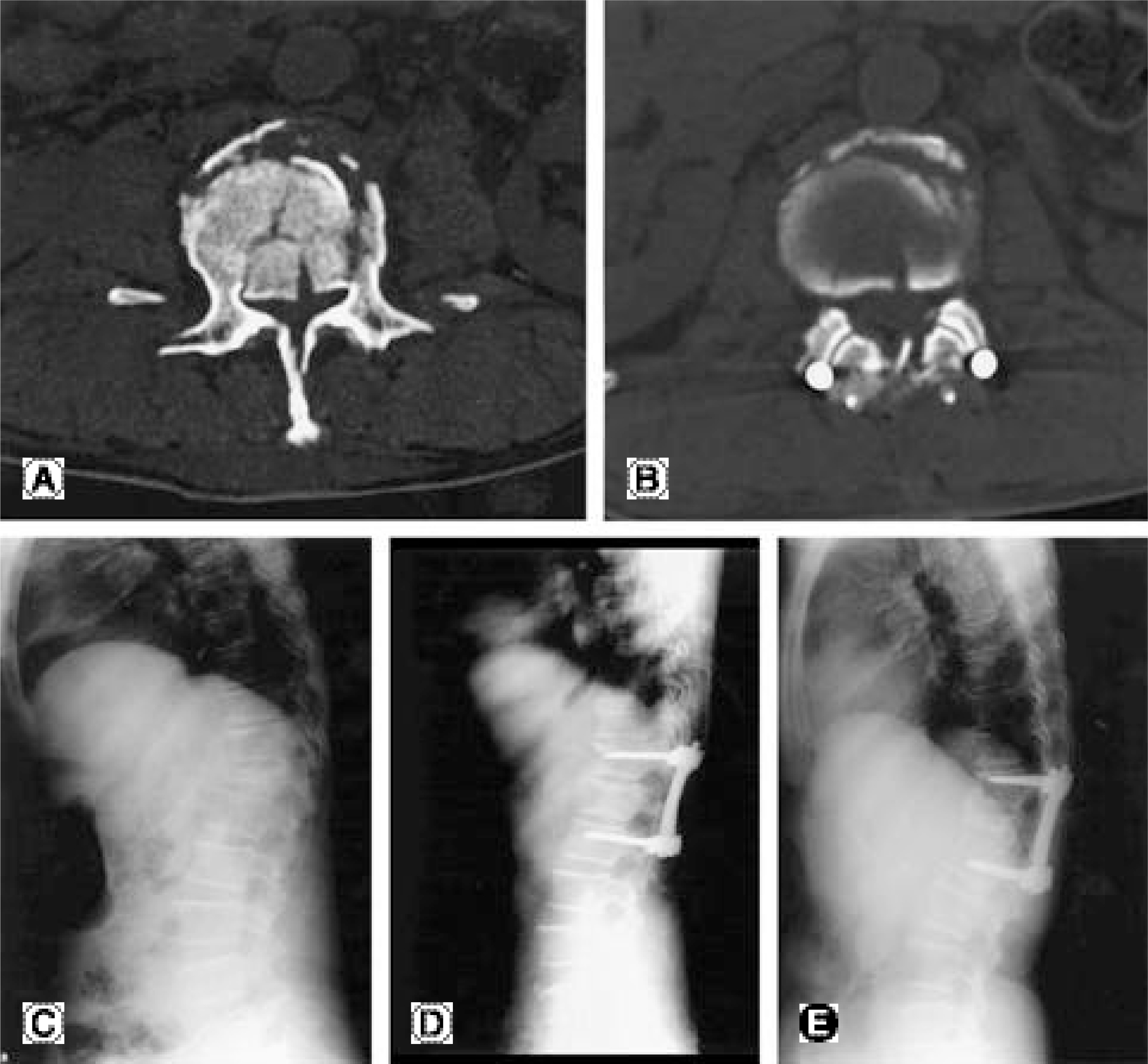
Fig. 2. Radiographs of a 36-year-old female with T12 unstable bursting fracture by fall from height. Initial Frankel grade was D. The fracture was Denis type A and 7 points in the McCormack's load sharing classification. (A) Preoperative axial CT scan shows 62% of the spinal canal occlusion. (B) Postoperative axial CT scan shows 24% of decompression. Frankel grade was improved into E. (C) Initial kyphotic angle is 29°. (D) Postoperative kyphotic angle is corrected up to 13°. (E) 3 years follow-up radiograph shows 28° of kyphotic angle. Correction loss is 15°.
Cited by 1 articles
-
Treatment Outcome of Lower Lumbar Fracture with Neurological Deficit
Hyeon Jun Kim, Kyu Yeol Lee, Min Soo Kang, Il Kwon Chung, Chul Won Lee, Dong Hoon Han
J Korean Soc Spine Surg. 2010;17(1):7-12. doi: 10.4184/JKSS.2010.17.1.7.
Reference
-
1). Floman Y, Farcy JPC, Argenson C. Thora co lumb ar spine fractures. 1st ed.New York: Raven Press;p. 251–306. 1993.2). Willen J, Lindahl F, Irstam L, Nordwall A. Unsta ble thoracolumbar fractures. A study by CT and conventional roentgenology of the reduction effect of harrington instrumentation. Spine. 1984; 9:214–219.3). Evart CM. Surgery of the musculoskeletal system. 2nd ed.New York: Churchill Livingstone Inc;p. 2161–2171. 1990.4). Denis F. The three column spine and its significance in the classification of acute thoracolumbar spine injuries. Spine. 1983; 8:817–831.5). Garfin SR, Mowery CA, Guerra J, Marshall LF. Con -firmation of the posterolateral technique to decompress and fuse thoracolumbar spine burst fractures. Spine. 1985; 10:218–223.6). Hashimoto T, Kaneda K, Abumi K. R e l a t i o ns h i p between traumatic spinal canal stenosis and neurological deficits in thoracolumbar burst fractures. Spine. 1988; 13:1268–1272.7). Kilcoyne RF, Mack LA, King HA, Ratcliffe SS, Loop JW. Thoracolumbar spinal injuries associated with vertebral plunges: Reappraisal with computed tomography. Radiology. 1983; 146:137–140.8). McAfee PG, Bohlman HH, Yuan HA. Anterior decompression of traumatic thoracolumbar fractures with incomplete neurological deficit using a retroperitoneal approach. J Bone Joint Surg Am. 1985; 67:89–104.
Article9). Kim NH, Lee HM, Chun IM. Neurologic injury and recovery in burst fracture of thoracolumbar spine. J Kor Spine Surg. 1995; 2:11–20.10). Kneene JS, Fischer SP, Vanderby R, Drumond DS, Turski PA. Significance of acute encroachment of the neural canal. Spine. 1989; 14:799–802.11). Frankel HL, Hancock DO, Hyslop G. The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. Paraplegia. 1969; 7:179–192.
Article12). McCormack T, Karaikovic E, Gaines RW. The load shearing classification of spine fractures. Spine. 1994; 19:1741–1744.13). Cobb RJ. Outline for the study of scoliosis. Am Acad Orthop Surg. 1948; 5:261–275.14). Gertzbein SD, Jacobs RR, Atoll J. Neurological outcome following surgery for spinal fractures. Spine. 1988; 13:892–895.15). Denis F. Spinal instability as defined by the three-column spine concept in acute spinal trauma: Clin Orthop. 1984. 65–76.16). McAfee PC, Yuan HA, Lasda NA. The unstable burst fracture: Spine. 1982; 7:365–373.17). Dekutoski MB, Conlan ES, Salciccioli GG. Spi n a l mobility and deformity after harrington rod stabilization and limited arthrodesis of thoracorumbar fractures. J Bone Joint Surg. 1993; 75:168–176.18). Muller U, Berlemann U, Sledge J, Schwarzenbach O. Treatment of thoracolumbar burst fractures without neurologic deficit by indirect reduction posterior instrumentation: bisegmental stabilization with monosegmental fusion. Eur Spine. 1999; 8:284–289.19). Carl AL, Tromanhauser SG, Roger DJ. Pedicle screw instrumentation for thoracolumbar burst fractures and fracture-dislocations. Spine. 1992; 17:317–324.
Article20). Ebelke DK, Asher MA, Neff JR, Kraker DP. Survivor -ship analysis of VSP spine instrumentation in the treatment of thoracolumbar and lumbar burst fractures. Spine. 1991; 16:428–432.21). Gurwitz GS, Dawson JM, McNamara MJ, Federspiel CF, Spengler DM. Biomechanical analysis of three surgical approaches for lumbar burst fractures using short-segment instrumentation. Spine. 1993; 18:997–982.
Article22). Lindsay RW, Dick W. The fixateur interne in the reduction and stabilization of thoracolumbar spine fractures in patients with neurologic deficit. Spine. 1991; 16:S140–5.
Article23). Parker JW, Lane JR, Karaikovic EE, Gaines RW. Successful short-segment instrumentation and fusion for thoracolumbar spine fractures. Spine. 2000; 25:1157–1169.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relationship between Canal Stenosis and Neurologic Deficits in Thoraco lumbar Burst Fracture
- Relationship between Simple X-ray and CT Findings on the Degree of Canal Encroachment in Burst Fracture of Thoracolumbar Junction
- Crush-Cleavage Fracture in Thoracolumbar and Lumbar Spine: Comparative Study with Type B Burst Fracture
- Relationship between Traumatic Spinal Canal Stenosis and Neurologic Deficits in Thoracolumbar Burst Fractures
- Relationship Between Degree of Spinal Canal Stenosis and Neurologic Deficits and Recovery in Thoracolumbar Burst Fractures
