Trapezoid Stress Fracture in a Weight Lifter
- Affiliations
-
- 1Department of Orthopedic Surgery, Pusan Paik Hospital, Inje University College of Medicine, Busan, Korea. honaud0@hanmail.net
- KMID: 2035873
- DOI: http://doi.org/10.4055/jkoa.2015.50.4.342
Abstract
- Trapezoid fracture is a rare condition and especially, isolated trapezoid fracture is most rare condition of carpal bone fracture. And principle of treatment has not yet been established. Most of trapezoid fractures can be treated using cast but displaced fracture or fracture combined with other carpal bone fractures may require operative treatment. There have been reports about case of conservative treatment in trapezoid stress fracture but no report about case of operative management. We treated a trapezoid stress fracture in a weight lifting athlete by operative treatment and report the results with literature review.
Keyword
Figure
-

Figure 1 Plain radiographs demonstrated increased trapezoid density with subchondral sclerosis.
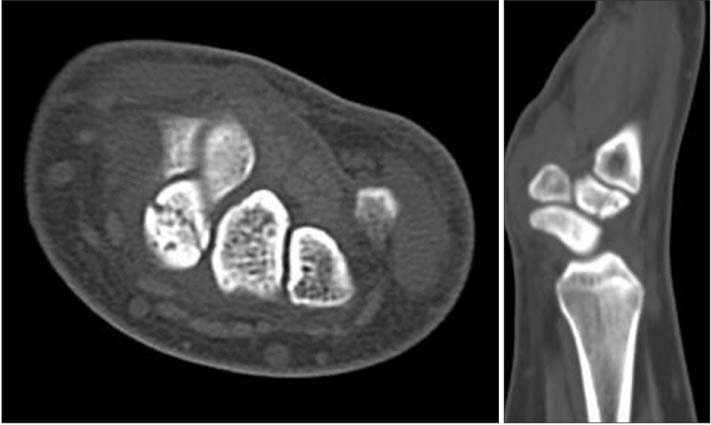
Figure 2 Computed tomography images demonstrated secondary changes. Subtle depressions, collapse and fragmentation.

Figure 3 Magnetic resonance imaging demonstrated wide areas of signal change including low signal intensity on proton density images and increased intensity on T2-weighted images, consistent with avascular necrosis.

Figure 4 Technetium-99m bone scintigraphy demonstrated moderate uptake of right trapezoid bone.

Figure 5 Computed tomography images after 6 weeks of conservative treatment showed no progression of union.

Figure 6 Using a dorsal approach, the fracture site was easily exposed. After removal of a necrotized lesion and confirmed bleeding of fracture surface, autologous bone graft was done. Serial open reduction and internal fixation with screw was performed.

Figure 7 Computed tomography images 6 months after the operation. Note the formation of bony callus.

Figure 8 Computed tomography images 10 months after the operation. Note the progression of bony uinion.
Reference
-
1. Papp S. Carpal bone fractures. Orthop Clin North Am. 2007; 38:251–260.
Article2. Sadowski RM, Montilla RD. Rare isolated trapezoid fracture: a case report. Hand (N Y). 2008; 3:372–374.
Article3. Afifi N, Lu JJ. A rare isolated trapezoid fracture. West J Emerg Med. 2011; 12:523–524.
Article4. Welling RD, Jacobson JA, Jamadar DA, Chong S, Caoili EM, Jebson PJ. MDCT and radiography of wrist fractures: radiographic sensitivity and fracture patterns. AJR Am J Roentgenol. 2008; 190:10–16.
Article5. Gruson KI, Kaplan KM, Paksima N. Isolated trapezoid fractures: a case report with compilation of the literature. Bull NYU Hosp Jt Dis. 2008; 66:57–60.6. Kain N, Heras-Palou C. Trapezoid fractures: report of 11 cases. J Hand Surg Am. 2012; 37:1159–1162.
Article7. Heron N, Verdugo F, Turmo A, Perez LT. Trapezoid stress fracture in an international shot-putter: a case report. J Sports Sci Med. 2012; 11:768–770.8. Miyawaki T, Kobayashi M, Matsuura S, Yanagawa H, Imai T, Kurihara K. Trapezoid bone fracture. Ann Plast Surg. 2000; 44:444–446.
Article9. D'Agostino P, Townley WA, Roulot E. Bilateral avascular necrosis of the trapezoid. J Hand Surg Am. 2011; 36:1678–1680.10. Gelberman RH, Gross MS. The vascularity of the wrist. Identification of arterial patterns at risk. Clin Orthop Relat Res. 1986; 202:40–49.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Dorsal Dislocation of the Trapezoid
- Fracture of Capitellum Humeri in Weight Lifting Athlete: A Case Reprt
- Stress Fracture on the 4th Metatarsal Bone after Treatment of Stress Fracture on the 5th Metatarsal Bone: A Case Report
- Design and Development of an Ergonomic Trolley-Lifter for Sheet Metal Handling Task: A Preliminary Study
- Subcapital Stress Fracture of the Femur after Internal Fixation of Intertrochanteric Fracture: A case report
