Korean Circ J.
2007 Aug;37(8):348-352. 10.4070/kcj.2007.37.8.348.
Pulmonary Atresia with Ventricular Septal Defect and Major Aorto-Pulmonary Collateral Arteries: Management Strategy at Our Hospital and the Results
- Affiliations
-
- 1Department of Pediatrics, College of Medicine, Seoul National University, Seoul, Korea. choi3628@snu.ac.kr
- 2Department of Pediatric Thoracic Surgery, College of Medicine, Seoul National University, Seoul, Korea.
- KMID: 2029061
- DOI: http://doi.org/10.4070/kcj.2007.37.8.348
Abstract
-
BACKGROUND AND OBJECTIVES: Based on our previous studies on pulmonary atresia with ventricular septal defect (VSD) and major aorto-pulmonary collateral arteries (MAPCAs), a management strategy for this disease was formulated at our hospital in 1999. To evaluate this strategy, it was applied to the new patients and their outcomes were measured.
SUBJECTS AND METHODS
The subjects were a cohort of newly diagnosed patients who were without any prior interventions and these patients were treated at our hospital from January 2000 to December 2003. The management strategy focused on promoting the growth of the pulmonary arterial confluence (PAC), if present, by performing a right ventricle-pulmonary artery conduit operation (RV-PA conduit). If the PAC was large or absent, then the management plan was discussed among the surgeons after performing an exhaustive work-up.
RESULTS
Seventeen patients were enrolled and their age at the time of diagnosis ranged from 8 days to 34 months with a median age of 3 months. The initial surgical method varied from one-stage total correction (4 cases) to a conduit operation with or without additional MAPCAs procedures (13 cases). All but three of the patients survived their initial surgery. There were two late deaths. In addition to the 3 survivors from one-stage total correction, 4 patients underwent a staged total corrective operation. The 5 remaining patients are still a subtotal correction state or a palliated state.
CONCLUSION
When a large PAC is present, one-stage total correction is the best surgical option. However, when the PAC is small, then RV-PA conduit without any vascular procedures may be a good alternative. This staged approach makes a larger PAC, which enables surgeons to create a much easier vascular anastomosis later on.
MeSH Terms
Figure
-
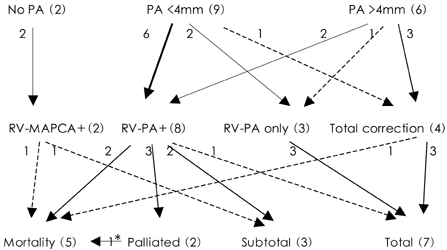
Fig. 1 Flow diagram by the size of the pulmonary artery and the first surgery. *: Medical death. RV-MAPCAs+: RV-Neo PA-MAPCAs with other MAPCAs procedures. RV-PA+: RV-PA conduit op. with other MAPCAs procedures.
Reference
-
1. Ramsay JM, Macartney FJ, Haworth SG. Tetralogy of Fallot with major aortopulmonary collateral arteries. Br Heart J. 1985. 53:167–172.2. Faller K, Haworth SG, Taylor JF, Macartney FJ. Duplicate sources of pulmonary blood supply in pulmonary atresia with ventricular septal defect. Br Heart J. 1981. 46:263–268.3. Choi JY, Yun YS. Diagnosis and management of pulmonary arteries with major aorto-pulmonary collateral arteries. Korean Circ J. 1989. 19:473–482.4. Millikian JS, Puga FJ, Danielson GK, Schaff HV, Julsrud PR, Mair DD. Staged surgical repair of pulmonary atresia, ventricular septal defect, and hypoplastic, confluent pulmonary arteries. J Thorac Cardiovasc Surg. 1986. 91:818–825.5. Puga FJ, Leoni FE, Julsrud PR, Mair DD. Complete repair of pulmonary atresia, ventricular septal defect and severe peripheral arborization abnormalies of the central pulmonary arteries: experience with preliminary unifocalization procedures in 38 patients. J Thorac Cardiovasc Surg. 1989. 98:1018–1029.6. Marelli AJ, Perloff JK, Child JS, Laks H. Pulmonary atresia with ventricular septal defect in adult. Circulation. 1994. 89:243–251.7. Sullivan ID, Wren C, Stark J, de Leval MR, Macartney FJ, Deanfield JE. Surgical unifocalization in pulmonary atresia and ventricular septal defect: a realistic goal? Circulation. 1988. 78:III5–III13.8. Permut LC, Laks H. Surgical management of pulmonary atresia with ventricular septal defect and multiple aortopulmonary collaterals. Adv Card Surg. 1994. 5:75–95.9. Dinarevic S, Redington A, Rigby M, Shinebourne EA. Outcome of pulmonary atresia and ventricular septal defect during infancy. Pediatr Cardiol. 1995. 16:276–282.10. Reddy VM, Petrossian E, McElhinney DB, Moore P, Teitel DF, Hanley FL. One stage complete unifocalization in infants: when should the ventricular septal defect be closed? J Thorac Cardiovasc Surg. 1997. 113:858–868.11. Tchervenkov CI, Salasidis G, Cecere R, et al. One-stage midline unifocalization and complete repair in infancy versus multiple-stage uniforcalization followed by repair for complex heart disease with major aortopulmonary collaterals. J Thorac Cardiovasc Surg. 1997. 114:727–737.12. Carotti A, Di Donato RM, Squitieri C, Guccione P, Catena G. Total repair of pulmonary atresia with ventricular septal defect and major aortopulmonary collaterals: an integrated apporach. J Thorac Cardiovasc Surg. 1998. 116:914–923.13. Iyler KS, Mee RB. Staged repair of pulmonary atresia with ventricular septal defect and major systemic to pulmonary artery collaterals. Ann Thorac Surg. 1991. 51:65–72.14. Sullivan ID, Stark J, deLeval M, Macartney FJ, Deanfield JE. Surgical unifocalization in pulmonary atresia with ventricular septal defect an major aortopulmonary collateral arteries. Circulation. 1988. 78:suppl III. III5–III13.15. Choi JY, Yu JY, Zhu L, et al. Ventricular septal defect and pulmonary atresia with major aorto-pulmonary collateral artery: diagnosis, management and review. J Korean Pediatr Cardiol Soc. 2006. 10:171–182.16. Choi JY, Lee JK, Cha ES, Sul JH, Lee SK, Choe KO. Origins, distributions and characteristics of collateral circulation in pulmonary atresia with ventricular septal defect. Korean Circ J. 1998. 28:1561–1576.17. Rome JR, Mayer JE, Castaneda AR, Lock JE. Tetralogy of Fallot with pulmonary atresia: rehabilitation of diminuitve pulmonary arteries. Circulation. 1993. 88:1691–1698.18. Haworth SG. Collateral arteries in pulmonary atresia with ventricular septal defect: a precarious blood supply. Br Heart J. 1980. 44:5–13.19. Piehler JM, Danielson GK, McGoon DC, Wallace RB, Fulton RE, Mair DD. Management of pulmonary atresia with ventricular septal defect and hypoplastic pulmonary arteries by right ventricular outflow construction. J Thorac Cardiovasc Surg. 1980. 80:552–567.20. Freedom RM, Pongiglioni G, Williams WG, Trusler GA, Rowe RD. Palliative right ventricular outflow reconstruction for patients with pulmonary atresia, ventricular septal defect, and hypoplastic pulmonary arteries. J Thorac Cardiovasc Surg. 1983. 86:24–36.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary Atresia with Ventricular Septal Defect and Major Aortopulmonary Collaterals Associated with Left Pulmonary Artery Interruption
- The major aortopulmonary collateral arteries in pulmonary atresia with ventricular septal defect: chest radiologic findings
- Ventricular Septal Defect and Pulmonary Atresia with Major Aorto-Pulmonary Collateral Artery: Diagnosis, Management and Review
- Diagnosis and Management of Pulmonary Atresia with Major Aorto-Pulmonary Collateral Arteries
- A case report of pulmonary atresia with pulmonary artery, PDA and ventricular septal defect
