Sciatic Nerve Compression Secondary Due to Ischial Tuberosity Osteochondroma
- Affiliations
-
- 1Department of Orthopedic Surgery, College of Medicine, Dong-A University, Busan, Korea. hyeonjun@dau.ac.kr
- KMID: 2014900
- DOI: http://doi.org/10.5371/jkhs.2012.24.1.65
Abstract
- Ostehochondroma is a common primary benign bone tumor, and is mostly asymptomatic. Symptoms are related complications due to compression on the adjacent nerve. The sciatic nerve compression secondary to osteochondroma has rarely been reported. A 21 year-old man had right hip pain radiated to the right lower extremity. In a radiological evaluation, bone mass was detected at the right ischial tuberosity. After dynamic ultrasonography, we excised the bone mass and decompressed the sciatic nerve. The bone mass was diagnosed as osteochondroma by pathologic evaluation. We report the case with a review of the literature.
Figure
-

Fig. 1 Preoperative radiographs. (A) Simple radiograph shows exophytic mass lesion with cortical expansion around right ischial tuberosity. (B) Computed tomograph shows exophytic mass lesion with cortical expansion around right ischial tuberosity and the mass narrows space between ischium and femoral neck. (C), (D) Magnetic resonance images show the same appearance with the simple radiograph and computed tomograph. The mass lesion shows isointense signal compared with nearby bone by both T1 and T2 weighted image. There is no evidence of sciatic nerve compression.
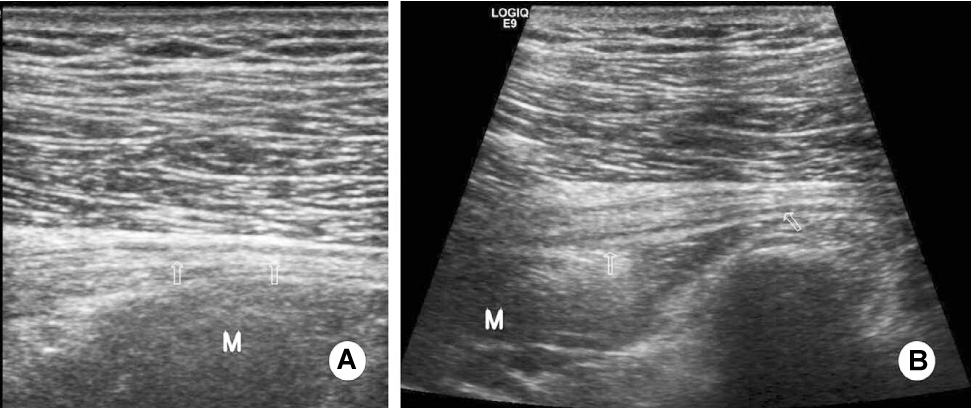
Fig. 2 Preoperative musculoskeletal Ultrasonogram. (A) The sciatic nerve is visualized and the gap between the sciatic nerve and bony mass is identified in preoperative musculoskeletal sono with prone position. (B) The sciatic nerve is not visualized and gap is not identified in hip flexion position. Arrows indicates the sciatic nerve. Capital M indicates the hypoechoic bone mass lesion.
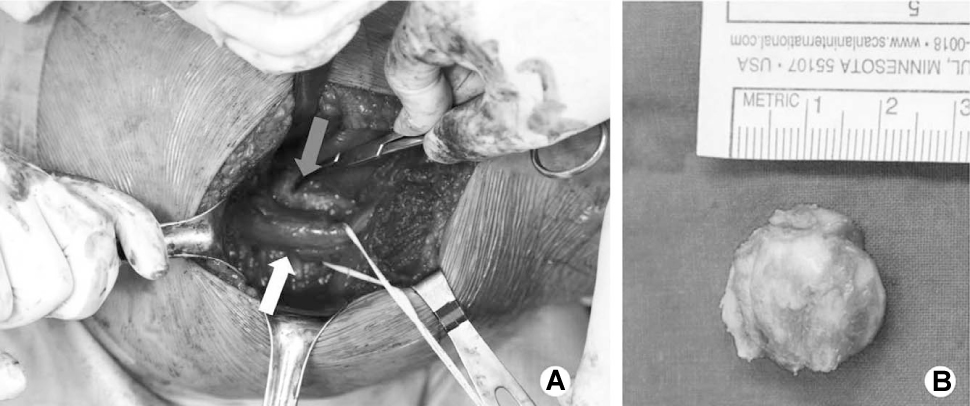
Fig. 3 Clinical photographs. (A) Intraoperative photograph shows osteochondroma of ischial tuberosity compressed the sciatic nerve which was swellen. Gray arrow indicates bony mass of ischial tuberosity. White arrow indicates the sciatic nerve. (B) Grossly, mass up to 2.5×1.8 cm were submitted. The specimen showed cancellous bone covered with cartilage cap, 0.25 cm in greatest thickness.

Fig. 4 Postoperative simple radiogrpah shows mass around right ischial tuberosity removed. Excision of the lesion resulted in complete relief of the patient's symptoms after 6 months.
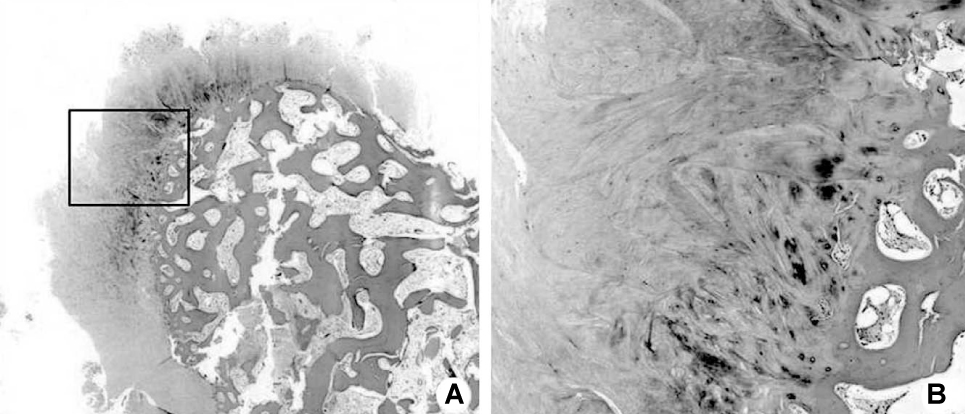
Fig. 5 Low-power (A: H-E stain, ×40) and high-power histologic examinations (B: H-E stain, ×100, black rectangular box of A) reveals mature bone covered with well deffierentiated cartilagenous cap. The chondrocytes of hyaline cartilage cap showed no cellular atypism.
Cited by 1 articles
-
The Optimal Surgical Approach and Complications in Resecting Osteochondroma around the Lesser Trochanter
Dae-Geun Jeon, Wan Hyeong Cho, Won Seok Song, Chang-Bae Kong, Seung Yong Lee, Do Yup Kim
J Korean Orthop Assoc. 2017;52(1):33-39. doi: 10.4055/jkoa.2017.52.1.33.
Reference
-
1. Peterson HA. Multiple hereditary osteochondromata. Clin Orthop Relat Res. 1989. 239:222–230.
Article2. Milgram JW. The origins of osteochondromas and enchondromas. A histopathologic study. Clin Orthop Relat Res. 1983. 174:264–284.3. Vasseur MA, Fabre O. Vascular complications of osteochondromas. J Vasc Surg. 2000. 31:532–538.
Article4. Kulcu DG, Naderi S. Differential diagnosis of intraspinal and extraspinal non-discogenic sciatica. J Clin Neurosci. 2008. 15:1246–1252.
Article5. Paik NJ, Han TR, Lim SJ. Multiple peripheral nerve compression related to malignantly transformed hereditary multiple exostoses. Muscle Nerve. 2000. 23:1290–1294.
Article6. Turan Ilica A, Yasar E, Tuba Sanal H, Duran C, Guvenc I. Sciatic nerve compression due to femoral neck osteochondroma: MDCT and MR findings. Clin Rheumatol. 2008. 27:403–404.
Article7. Sherman PM, Matchette MW, Sanders TG, Parsons TW. Acetabular paralabral cyst: an uncommon cause of sciatica. Skeletal Radiol. 2003. 32:90–94.
Article8. Kim S, Choi JY, Huh YM, et al. Role of magnetic resonance imaging in entrapment and compressive neuropathy - what, where, and how to see the peripheral nerves on the musculoskeletal magnetic resonance image: part 1. Overview and lower extremity. Eur Radiol. 2007. 17:139–149.
Article9. Grant GA, Britz GW, Goodkin R, Jarvik JG, Maravilla K, Kliot M. The utility of magnetic resonance imaging in evaluating peripheral nerve disorders. Muscle Nerve. 2002. 25:314–331.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sciatic Nerve Compression due to Ganglion
- Sequela of Untreated Avulsion Fracutre of Ischial Tuberosity: Report of Two Cases
- Bilateral Sciatic Neuropathy associated with Rhabdomyolysis in an Immobilized Patient: A case report
- Sciatic Nerve Compression in a Patient with Pesistent Sciatic Artery: A Case Report
- Cubital Tunnel Syndrome Caused by Osteochondroma: A Case Report
