J Lipid Atheroscler.
2015 Jun;4(1):35-38. 10.12997/jla.2015.4.1.35.
Complex Coronary Artery Fistula Causing Angina is Resolved Through Coil Embolization
- Affiliations
-
- 1Department of Internal Medicine and Cardiovascular Center, Seoul National University Hospital, Seoul, Korea. hylee612@snu.ac.kr
- KMID: 2005733
- DOI: http://doi.org/10.12997/jla.2015.4.1.35
Abstract
- Coronary artery fistulas (CAFs) are rare, mostly congenital cardiac anomalies. Most are asymptomatic and do not require treatment, but some can cause angina or exertional dyspnea. Symptomatic or hemodynamically significant fistulae can be treated with transcatheter or surgical methods of closure, with the former being a less invasive alternative while showing similar effectiveness and morbidity. We present a 52-year-old man with a complex coronary artery to pulmonary artery fistula causing angina, successfully treated by transcatheter coil embolization. Even without complete closure, this patient showed improvement of symptoms and objective indices of myocardial ischemia.
Keyword
MeSH Terms
Figure
-

Fig. 1 Coronary CT angiography shows fistulae originating from (A) the proximal right coronary artery (RCA), (B) left main coronary artery (LMCA), and ascending aorta near the LMCA. The fistulae drain into the left side of the main pulmonary trunk.
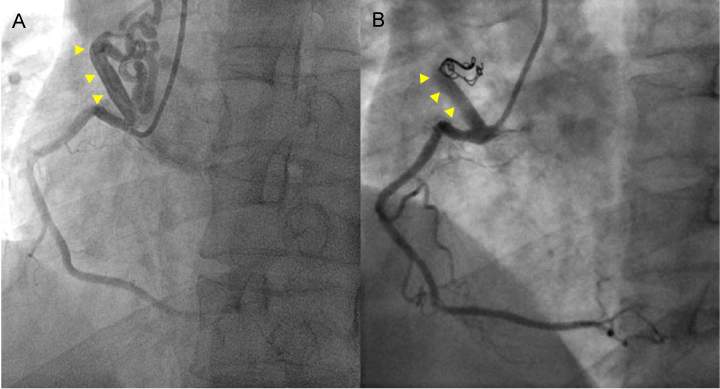
Fig. 2 Coronary angiography shows (A) the right coronary-to-pulmonary artery fistula, (B) Selective embolization with coiling was performed.
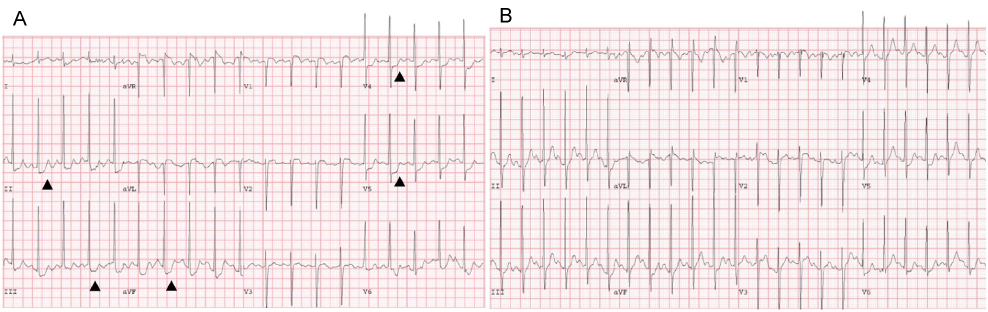
Fig. 3 (A) Pre-procedural treadmill test (TMT) shows ST depression at leads II, III, aVF, V4, V5 (black arrows), suggesting myocardial ischemia, (B) TMT six months later shows no signs of myocardial ischemia.
Reference
-
1. Dodge-Khatami A, Mavroudis C, Backer CL. Congenital heart surgery nomenclature and database project: anomalies of the coronary arteries. Ann Thorac Surg. 2000; 69:S270–S297.
Article2. Mangukia CV. Coronary artery fistula. Ann Thorac Surg. 2012; 93:2084–2092.
Article3. Fernandes ED, Kadivar H, Hallman GL, Reul GJ, Ott DA, Cooley DA. Congenital malformations of the coronary arteries: the Texas Heart Institute experience. Ann Thorac Surg. 1992; 54:732–740.
Article4. Ata Y, Turk T, Bicer M, Yalcin M, Ata F, Yavuz S. Coronary arteriovenous fistulas in the adults: natural history and management strategies. J Cardiothorac Surg. 2009; 4:62.
Article5. Armsby LR, Keane JF, Sherwood MC, Forbess JM, Perry SB, Lock JE. Management of coronary artery fistulae. Patient selection and results of transcatheter closure. J Am Coll Cardiol. 2002; 39:1026–1032.
Article6. Onorati F, Mastroroberto P, Bilotta M, Cristodoro L, Esposito A, Pezzo F, et al. Surgical treatment of coronary-to-pulmonary fistula: how and when? Heart Vessels. 2006; 21:321–324.
Article7. Taleb MM, Sheikh MA, Cooper CJ, Tinkel JL. Multiple coronary to pulmonary artery fistulas: a case report and review of the literature. Cardiovasc Interv Ther. 2012; 27:127–130.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Percutaneous Transcatheter Coil Embolization for Congenital Coronary Arteriovenous Fistula
- A Case of Giant Aneurysm of Coronary Arteriovenous Fistula Treated by Percutaneous Deployment of Embolization Coil
- Transcatheter Coil Closure of a Congenital Coronary Arterial Fistula
- Transcatheter Coil Embolization of Coronary Arteriovenous Fistula in Patient with Turner Phenotype with 46,XX
- Coronary Artery Fistula with Giant Aneurysm and Coronary Stenosis Treated by Transcatheter Embolization and Stent
