J Korean Surg Soc.
2009 Sep;77(3):221-224. 10.4174/jkss.2009.77.3.221.
Post-traumatic Lumbar Hernia Repaired with PHS (Prolene Hernia System)
- Affiliations
-
- 1Department of Surgery, Gil Hospital, Gachon University of Medicine and Science, Incheon, Korea. mc@gilhospital.com
- KMID: 2004224
- DOI: http://doi.org/10.4174/jkss.2009.77.3.221
Abstract
- Lumbar hernia is a rare disease. Only five papers on lumbar hernia are found in the Journal of the Korean Surgical Society. Lumbar hernia is an extrusion of intraperitoneal or extraperitoneal organs of the abdomen through a defect of the transversalis fascia or the transversus abdominis muscle aponeurosis in the posterolateral abdominal wall. The most frequent symptom of this hernia is a protruding mass at the lateral abdominal wall with increased abdominal pressure. I encountered a case of lumbar hernia. The subject fell off of a subway platform. The cervical spine was injured and he suffered from quadriplegia. After several operations, he recovered from the quadriplegia. Following that, he discovered a left lumbar mass, incidentally. CT and MRI revealed this mass to be a Grynfeltt's hernia. This hernia was corrected by open method with PHS. There were no complications or discomfort after the operation. I report this case with a review of the literature.
Keyword
MeSH Terms
Figure
-
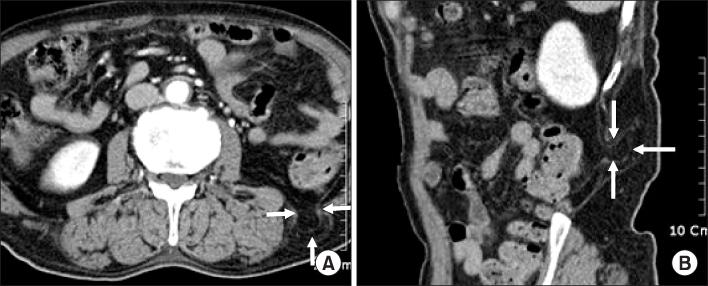
Fig. 1 CT findings of lumbar hernia. Defect (arrows) is shown between quadratus lumborum muscle and internal oblique muscle This finding means this defect is Gynfeltt's lumbar hernia.
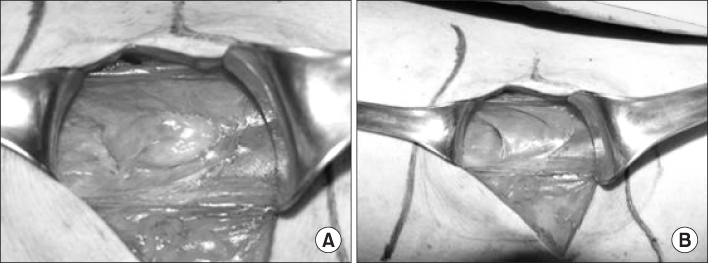
Fig. 2 Operation findings of lumbar hernia. Fat is protruded through defect (B). There is a 1 cm in diameter- sized defect after reduction (A). Line on left side is costal margin and line on right side is iliac crest.

Fig. 3 Operation field after insertion of PHS (prolene hernia system). Onlay is removed and four stitches are applied to fix the PHS. Line on left side is costal margin and Line on right side is iliac crest.
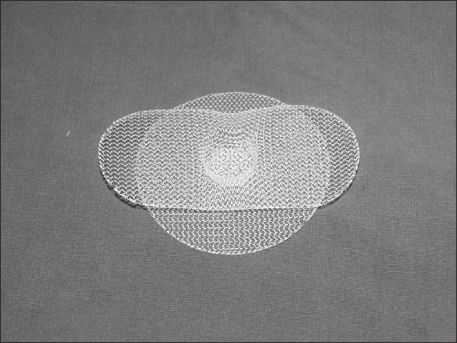
Fig. 4 PHS (medium size). PHS has three components; onlay, underlay and connector.
Reference
-
1. Skrekas G, Stafyla VK, Papalois VE. A Grynfeltt hernia: report of a case. Hernia. 2005. 9:188–191.2. Moreno-Egea A, Baena EG, Calle MC, Martinez JA, Albasini JL. Controversies in the current management of lumbar hernias. Arch Surg. 2007. 142:82–88.3. Armstrong O, Hamel A, Grignon B, NDoye JM, Hamel O, Robert R, et al. Lumbar hernia: anatomical basis and clinical aspects. Surg Radiol Anat. 2008. 30:533–537.4. Salameh JR. Primary and unusual abdominal wall hernias. Surg Clin North Am. 2008. 88:45–60.5. Park HR, Baek SK, Lee TS, Bae OS, Park SD. Lumbar hernia combined with descending colon incarceration. J Korean Surg Soc. 2006. 71:482–485.6. Shin DJ, Kim W, Lee DS, Song MH, Sung KY, Park IY, et al. Superior lumbar hernia: a case report. J Korean Surg Soc. 1999. 56:1052–1054.7. Moreno-Egea A, Torralba-Martinez JA, Morales G, Fernandez T, Girela E, Aguayo-Albasini JL. Open vs laparoscopic repair of secondary lumbar hernias: a prospective nonrandomized study. Surg Endosc. 2005. 19:184–187.8. Zhou X, Nve JO, Chen G. Lumbar hernia: clinical analysis of 11 cases. Hernia. 2004. 8:260–263.9. Losanoff JE, Kjossev KT. Diagnosis and treatment of primary incarcerated lumbar hernia. Eur J Surg. 2002. 168:193–195.10. Khera G, Berstock DA. Incisional, epigastric and umbilical hernia repair using the Prolene Hernia System: describing a novel technique. Hernia. 2006. 10:367–369.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Traumatic Lumbar Hernia: Report of a Case
- Comparing of Complications of Inguinal Hernia Repair Using Prolene Hernia System
- 120 Cases of Hernia Repair with Bilayer Patch (Prolene Hernia System)
- Comparison of Three Types of Hernioplasty Using Meshes for Adult Inguinal Hernia: Lichtenstein, Mesh-plug, Prolene Hernia System
- A Tension-free Herniorrhaphy Using the Prolene Hernia System: Clinical Experiences
