C1-2 Transarticular Screw Fixation as a Revision Surgery for Failed C1-2 Fusion: Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, School of Medicine, Kyunghee University, Seoul, Korea. sks111@khmc.or.kr
- KMID: 2003233
- DOI: http://doi.org/10.4184/jkss.2002.9.3.251
Abstract
- Odontoid process fracture, nonunion or atlantoaxial instability are generally treated with posterior fusion using sublaminar wiring techinique. And occiput to C2 fusion is performed in cases with posterior arch defect of atlas. However, occiput to C2 fusion can not stabilize unstable C1-2 segment before accomplishment of fusion. Therefore, postoperative external support is necessary. A 48-year old male patient visited our hospital due to weakness and spasticity of four extremities. 6 months ago, he got C1-2 fusion in other university hospital due to odontoid process fracture. 6 months after surgery, sublaminar cable was pulled out and grafted bone was absorbed. The neurological deficits were worsened(spasticity of four extremities with severe myelopathy, bed ridden state). JOA score was 4. Diagnosis of the patient was C1-2 instability with cervical myelopathy due to odontoid process fracture nonunion and posterior arch defect of atlas. C1-2 transarticular screw fixation and occiput to C2 fusion were performed.
MeSH Terms
Figure
-

Fig. 1. Preoperative lateral radiography of the cervical spine shows odontoid process fracture of the axis with anterior subluxation of the atlas (A). Postoperative lateral radiography of the cervical spine shows Brooks wiring and fusion of C1-2 and good reduction of atlas (B).
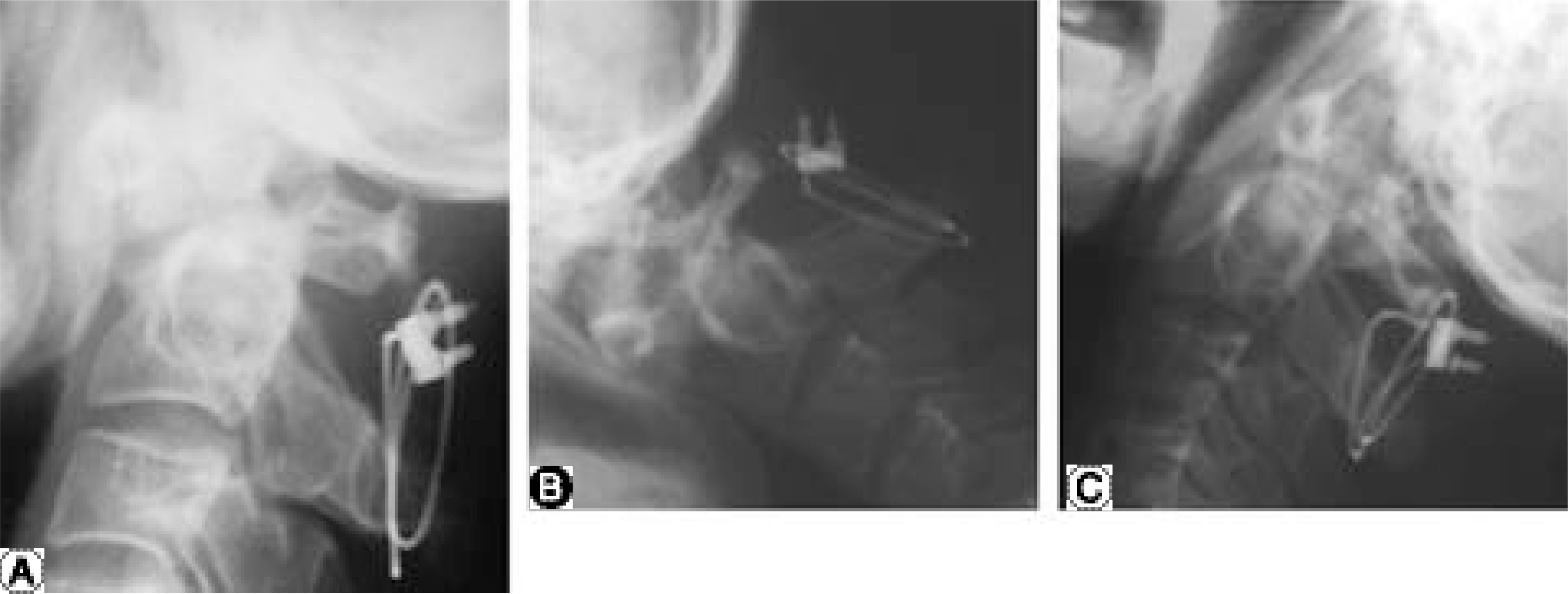
Fig. 2. Lateral radiography of cervical spine at six months after surgery shows pulled-out sublaminar wire, loss of reduction, absorption of grafted bone (A). Flexion and extension lateral radiography of cervical spine shows instability of the C1-2 segment (B, C).
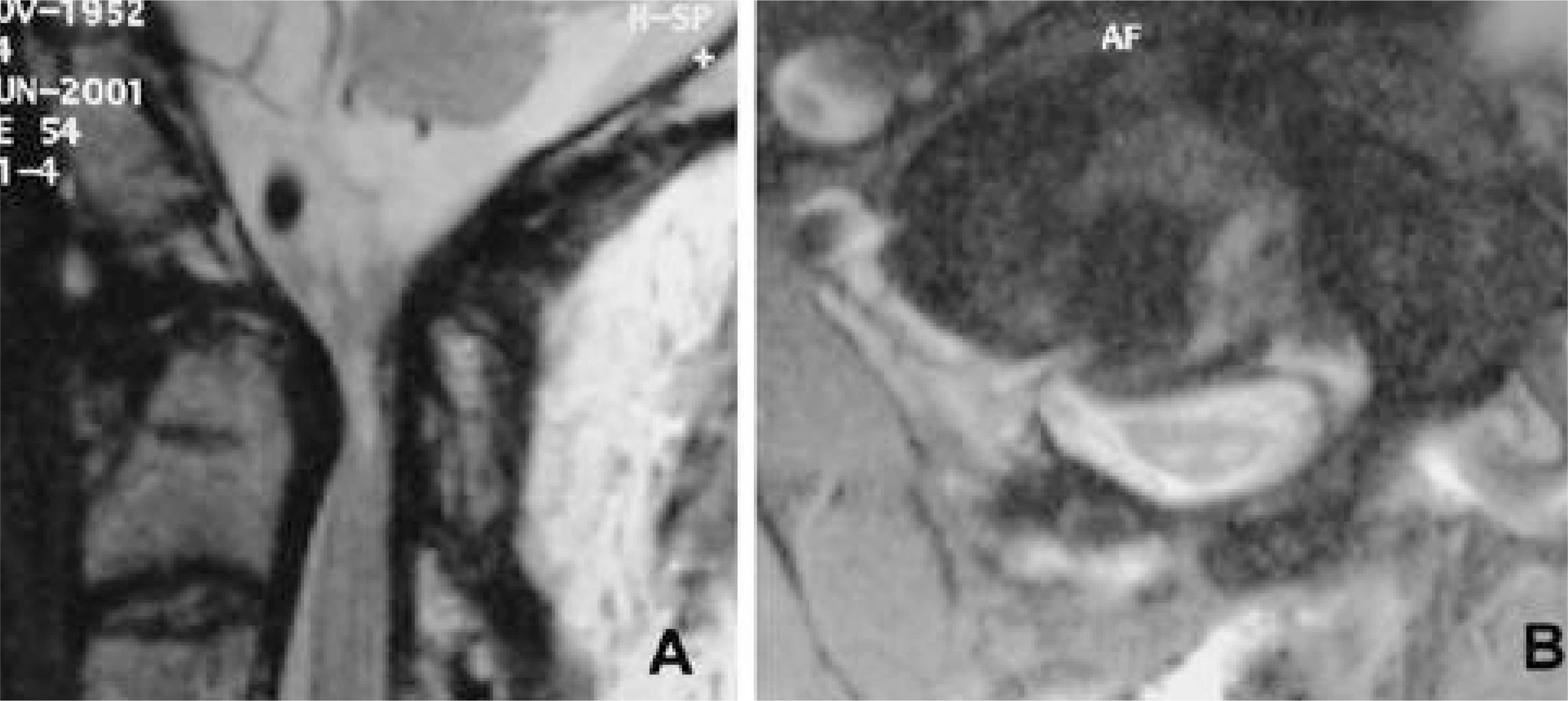
Fig. 3. T2-weighted sagittal magnetic resonance (MR) image of cervical spine shows compression of the spinal cord with high signal intensity in the cord (A). T2-weighted axial MR image of cervical spine shows marked compression of the spinal cord with defect in the posterior arch of the atlas (B).
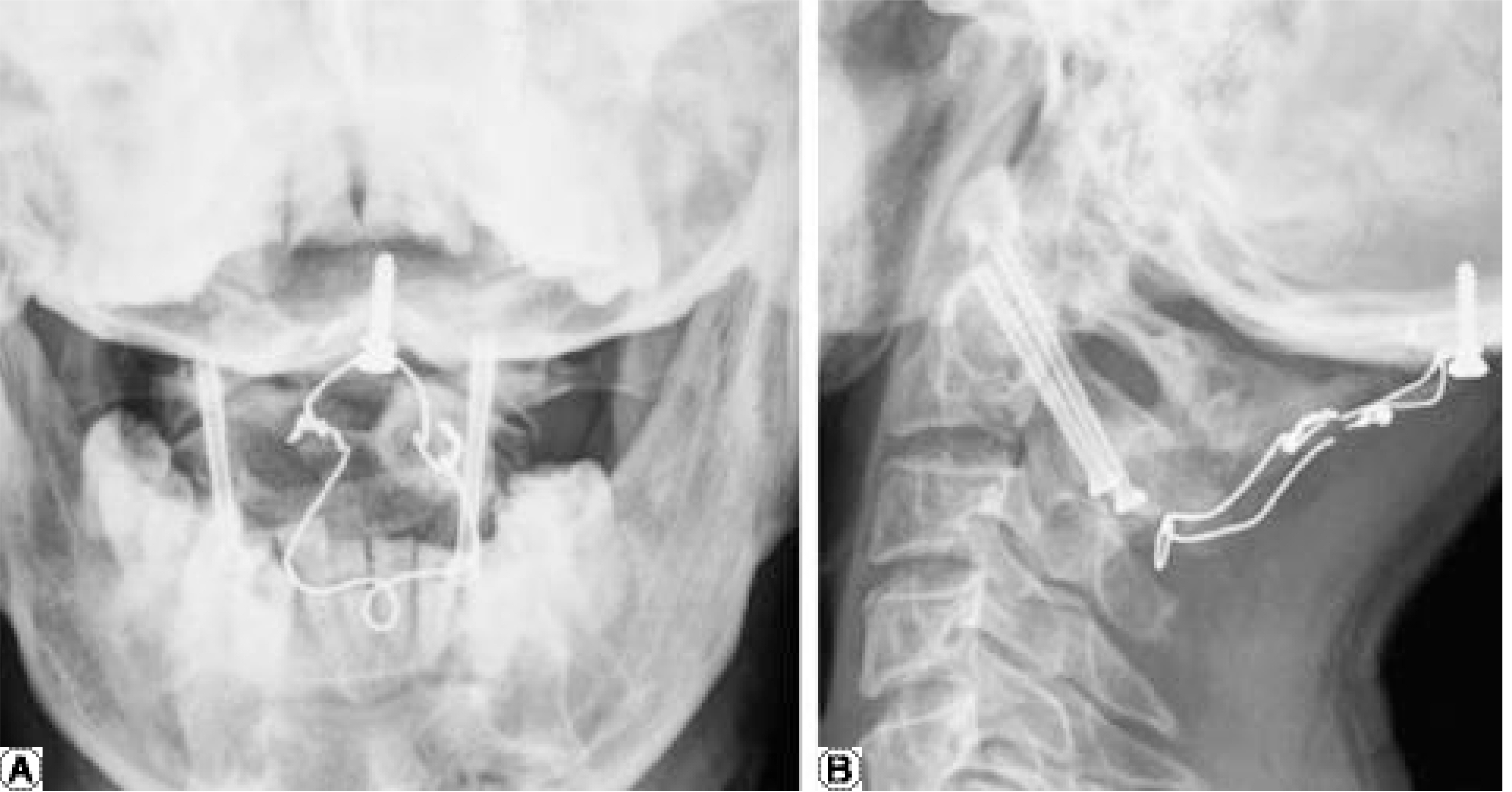
Fig. 4. Postoperative (revision C1-2 transarticular screw fixation) one-year followup radiography of the cervical spine. Open mouth view shows good reduction of the C1-2 segment and good purchase of C1-2 articulation with screws (A). Lateral radiography of the cervical spine shows good reduction of odontoid process and good bony fusion between the C1-2 segment (B).
Reference
-
1). Coric D, Branch CL, Wilson JA, Robinson JC. Art e-riovenous fistula as a complication of C1-2 transarticular screw fixation. Case report and review of the literature. J Neurosurg. 85(2):340–3. 1996.2). Dickman CA, Sonntag VK. Surgical management of atlantoaxial nonunion. J Neurosurg. 83(2):248–53. 1995.4). Grob D, Crisco J, Panjabi MM, Dvorak J. Biomechanical evaluation of four different posterior atlantoaxial fixation technique. Spine. 17:480–90. 1991.5). Grob D, Jeanneret B, Aebi M, Markwalder T. Atlantoaxial fusion with transarticular screw-fixation. J Bone Joint Surg. 73-B:972–6. 1991.6). Grob D, Magerl F. Surgical stabilization of C1 and C2 fractures. Orthopade. 16(1):46–54. 1987.7). Hurlbert RJ, Crawford NR, Choi WG, Dickman CA. A biomechanical evaluation of occipitocervical instrumentation: screw compared with wire fixation. J Neurosurg. 90(1 Suppl):84–90. 1999.
Article8). Jeanneret B, Magerl F. Primary posterior fusion C1/2 in odontoid fracture: indications, technique, and results of transarticular screw fixation. J Spinal Disord. 5(4):464–75. 1992.9). Kawaguchi Y, Ishihara H, Ohmoi K Kanamori M, Kimura T. Computer-assisted Magerl's transarticular screw fixation for atlantoaxial subluxation. J Orhop Sci. 7(1):131–6. 2002.
Article10). Knoringer P. Surgical treatment of injuries of the upper cervical spine. Langenbecks Arch Chir Suppl Kongressbd. 279-85:1992.11). Madawi AA, Casey AT, Solanki GA, Tuite G, Veres R, Crockard HA. Radiological and anatomical evaluation of the atlantoaxial transarticular screw fixation technique. J Neurosurg. 86(6):961–8. 1997.
Article12). Mizuno J, Nakagawa H. Spinal instrumentation for unstable C1-2 injury. Neurol Med Chir. 39(6):434–9. 1999.
Article13). Neo M, Matsushita M, Yasuda T, Sakamoto T, Na-kamura T. Use of an aiming device in posterior atlantoaxial transarticular screw fixation. Technical note. J Neurosurg. 97(1 Suppl):123–7. 2002.14). Paramore CG, Dickman CA, Sonntag VK. Th e anatomical suitability of the C1-2 complex for transarticular screw fixation. J Neurosurg. 85(2):221–4. 1996.15). Prabhu VC, France JC, Voelker JL, Zoarski GH. Vertebral artery pseudoaneurysm complicating posterior C1-2 transarticular screw fixation: case report. Surg Neurol. 55(1):29–34. 2001.
Article16). Song GS, Theodore N, Dickman CA, Sonntag VK. Unilateral posterior atlantoaxial transarticular screw fixation. J Neurosurg. 87(6):851–5. 1997.
Article17). Wright NM, Lauryssen C. Vertebral artery injury in C1-2 transarticular screw fixation: results of a survey of the AANS/CNS section on disorders of the spine and peripheral nerves. American Association of Neurological Surgeons/Congress of Neurological Surgeons. J Neurosurg. 88(4):636–40. 1998.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- C1/2 Transarticular Screw Fixation for Complicated Os Odontoideum: Case Report
- Posterior C1-2 Transarticular Screw Fixation in Atlantoaxial Instability
- Application of C1-C3 Halifax Interlaminar Clamps in Addition to C1-C2 Cable Fixation
- Long Term Follow up and Clinical Results of Posterior C1/2 Fixation
- Intraoperative Vertebral Artery Angiography to Guide C1-2 Transarticular Screw Fixation in a Patient with Athetoid Cerebral Palsy
