Proper Treatment of Acute Mesenteric Ischemia
- Affiliations
-
- 1Department of Radiology, Chonbuk National University Hospital and Medical School, Jeonju, Korea. ymhan@chonbuk.ac.kr
- 2Research Institute of Clinical Medicine, Chonbuk National University Hospital and Medical School, Jeonju, Korea.
- 3Department of Surgery, Chonbuk National University Hospital and Medical School, Jeonju, Korea.
- KMID: 2002935
- DOI: http://doi.org/10.3348/jksr.2011.65.4.345
Abstract
- PURPOSE
To evaluate the effectiveness of treatment options for Acute Mesenteric Ischemia and establish proper treatment guidelines.
MATERIALS AND METHODS
From January 2007 to May 2010, 14 patients (13 men and 1 woman, mean age: 52.1 years) with acute mesenteric ischemia were enrolled in this study. All of the lesions were detected by CT scan and angiography. Initially, 4 patients underwent conservative treatment. Eleven patients were managed by endovascular treatment. We evaluated the therapeutic success and survival rate of each patient.
RESULTS
The causes of ischemia included thromboembolism in 6 patients and dissection in 8 patients. Nine patients showed bowel ischemia on CT scans, 4 dissection patients underwent conservative treatment, 3 patients had recurring symptoms, and 5 dissection patients underwent endovascular treatment. Overall success and survival rate was 100%. However, overall success was 83% and survival rate was 40% in the 6 thromboembolism patients. The choice of 20 hours as the critical time in which the procedure is ideally performed was statistically significant (p = 0.0476).
CONCLUSION
A percutaneous endovascular procedure is an effective treatment for acute mesenteric ischemia, especially in patients who underwent treatment within 20 hours. However, further study and a long term follow-up are needed.
MeSH Terms
Figure
-

Fig. 1 71-year-old man suddenly experienced periumbilical pain. The symptom duration time was 18.5 hours. A. Contrast-enhanced CT scan shows free flap (arrow) in superior mesenteric artery with decreased small bowel enhancement (open arrow). B. On digital subtraction angiogram, there were narrowed true lumen of the superior mesenteric artery and a clearly visible dissection flap from 2 cm distal to the ostium (arrow). C. A 6 × 36-mm self-expandable Wallstent was placed in the true lumen. Final angiogram shows a patent true lumen with good blood flow in all the branches of the superior mesenteric artery. D. Contrast-enhanced CT at 1 month after the procedure shows good patency through the fully expanded stents with complete occlusion of the false lumen. The patient remained completely asymptomatic for 740 days.

Fig. 2 72-year-old who visited ER due to epigastric pain. The symptom duration time was 4 hours. A. Contrast-enhanced CT scan shows filling defect (open arrow) at the proximal portion of the SMA with decreased bowel enhancement. B. SMA arteriogram demonstrated thrombotic occlusion a few centimeters distal to the orifice. C. After continuous infusion of urokinase into the SMA, arteriogram revealed improved distal flow but, residual stenosis was seen (arrow). D. A 6 × 48-mm self-expandable Wallstent was placed in the stenotic segment. Final angiogram shows completely restored blood flow in the major branches of the SMA. E. CT scan showed ongoing patency of the SMA after 1 year. At 741 days follow-up period, the patient has not experienced recurrence of abdominal pain. Note.-ER = Emergency Room, SMA = superior mesenteric artery
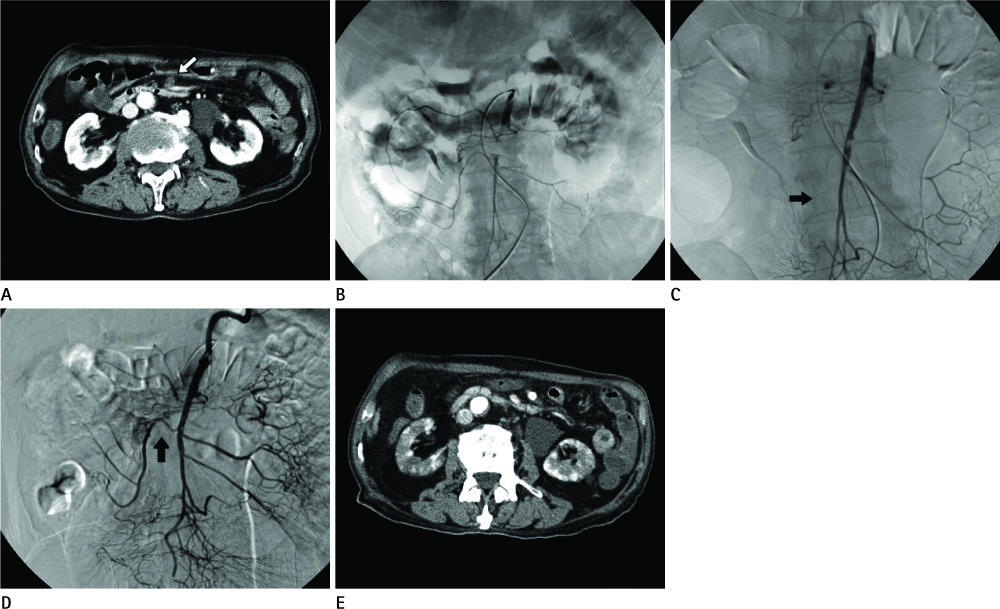
Fig. 3 79-year-old man who visited ER due to epigastric pain. His medical history included atrial fibrillation and hypertension. The symptom duration time was 31.5 hours. A. Contrast-enhanced CT scan shows filling defect (open arrow) at the proximal portion of the SMA without definitely decreased bowel enhancement. B. SMA arteriogram shows a complete thrombotic occlusion of the proximal portion of the main stem. C. A 6 × 29-mm self-expandable Wallstent was placed in the occlusive segment. But, Rt. colic artery was not visualized after procedure (arrow). D. We performed multiple courses of aspiration thrombectomy using a 6.0 Fr aspiration catheter after intra-arterial thrombolysis. Final angiogram shows a recanalized Rt. colic artery (arrow). E. Contrast-enhanced CT at 34 days after the procedure shows no filling defect in the SMA, but decreased small bowel enhancement and multifocal perfusion defect in both kidneys. He expired due to multi-organ failure. Note.-ER = Emergency Room, SMA = superior mesenteric artery
Reference
-
1. Mamode N, Pickford I, Leiberman P. Failure to improve outcome in acute mesenteric ischaemia: seven-year review. Eur J Surg. 1999; 165:203–208.2. Acosta S, Ogren M, Sternby NH, Bergqvist D, Björck M. Incidence of acute thrombo-embolic occlusion of the superior mesenteric artery--a population-based study. Eur J Vasc Endovasc Surg. 2004; 27:145–150.3. Brandt LJ, Boley SJ. AGA technical review on intestinal ischemia. American Gastrointestinal Association. Gastroenterology. 2000; 118:954–968.4. Acosta S. Epidemiology of mesenteric vascular disease: clinical implications. Semin Vasc Surg. 2010; 23:4–8.5. Leung DA, Schneider E, Kubik-Huch R, Marincek B, Pfammatter T. Acute mesenteric ischemia caused by spontaneous isolated dissection of the superior mesenteric artery: treatment by percutaneous stent placement. Eur Radiol. 2000; 10:1916–1919.6. Ambo T, Noguchi Y, Iwasaki H, Kondo J, Matsumoto A, Suzuki H, et al. An isolated dissecting aneurysm of the superior mesenteric artery: report of a case. Surg Today. 1994; 24:933–936.7. Ko GJ, Han KJ, Han SG, Hwang SY, Choi CH, Gham CW, et al. A case of spontaneous dissection of the superior mesenteric artery treated By percutaneous stent placement. Korean J Gastroenterol. 2006; 47:168–172.8. Casella IB, Bosch MA, Sousa WO Jr. Isolated spontaneous dissection of the superior mesenteric artery treated by percutaneous stent placement: case report. J Vasc Surg. 2008; 47:197–200.9. Edwards MS, Cherr GS, Craven TE, Olsen AW, Plonk GW, Geary RL, et al. Acute occlusive mesenteric ischemia: surgical management and outcomes. Ann Vasc Surg. 2003; 17:72–79.10. Kougias P, Lau D, El Sayed HF, Zhou W, Huynh TT, Lin PH. Determinants of mortality and treatment outcome following surgical interventions for acute mesenteric ischemia. J Vasc Surg. 2007; 46:467–474.11. Silva JA, White CJ, Collins TJ, Jenkins JS, Andry ME, Reilly JP, et al. Endovascular therapy for chronic mesenteric ischemia. J Am Coll Cardiol. 2006; 47:944–950.12. Gweon HM, Suh SH, Won JY, Lee DY, Kim SS. Percutaneous stenting of the superior mesenteric artery for the treatment of chronic mesenteric ischemia. J Korean Radiol Soc. 2008; 58:571–578.13. Demirpolat G, Oran I, Tamsel S, Parildar M, Memis A. Acute mesenteric ischemia: endovascular therapy. Abdom Imaging. 2007; 32:299–303.14. Gartenschlaeger S, Bender S, Maeurer J, Schroeder RJ. Successful percutaneous transluminal angioplasty and stenting in acute mesenteric ischemia. Cardiovasc Intervent Radiol. 2008; 31:398–400.15. Cortese B, Limbruno U. Acute mesenteric ischemia: primary percutaneous therapy. Catheter Cardiovasc Interv. 2010; 75:283–285.16. Acosta S, Sonesson B, Resch T. Endovascular therapeutic approaches for acute superior mesenteric artery occlusion. Cardiovasc Intervent Radiol. 2009; 32:896–905.17. Block TA, Acosta S, Björck M. Endovascular and open surgery for acute occlusion of the superior mesenteric artery. J Vasc Surg. 2010; 52:959–966.18. van der Worp HB, van Gijn J. Clinical practice. Acute ischemic stroke. N Engl J Med. 2007; 357:572–579.19. Lee DH, Na DG, Ihn YK, Kim DJ, Kim EY, Kim YS, et al. Review of the current status of intra-arterial thrombolysis for treating acute cerebral infarction: a retrospective analysis of the data from multiple centers in Korea. Korean J Radiol. 2007; 8:87–93.20. Adams HP Jr, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007; 38:1655–1711.21. Gouëffic Y, Costargent A, Dupas B, Heymann MF, Chaillou P, Patra P. Superior mesenteric artery dissection: case report. J Vasc Surg. 2002; 35:1003–1005.22. Yoon YW, Choi D, Cho SY, Lee DY. Successful treatment of isolated spontaneous superior mesenteric artery dissection with stent placement. Cardiovasc Intervent Radiol. 2003; 26:475–478.23. Sakamoto I, Ogawa Y, Sueyoshi E, Fukui K, Murakami T, Uetani M. Imaging appearances and management of isolated spontaneous dissection of the superior mesenteric artery. Eur J Radiol. 2007; 64:103–110.24. Morris JT, Guerriero J, Sage JG, Mansour MA. Three isolated superior mesenteric artery dissections: update of previous case reports, diagnostics, and treatment options. J Vasc Surg. 2008; 47:649–653.25. Takayama T, Miyata T, Shirakawa M, Nagawa H. Isolated spontaneous dissection of the splanchnic arteries. J Vasc Surg. 2008; 48:329–333.26. Gobble RM, Brill ER, Rockman CB, Hecht EM, Lamparello PJ, Jacobowitz GR, et al. Endovascular treatment of spontaneous dissections of the superior mesenteric artery. J Vasc Surg. 2009; 50:1326–1332.27. Subhas G, Gupta A, Nawalany M, Oppat WF. Spontaneous isolated superior mesenteric artery dissection: a case report and literature review with management algorithm. Ann Vasc Surg. 2009; 23:788–798.28. Yun WS, Kim YW, Park KB, Cho SK, Do YS, Lee KB, et al. Clinical and angiographic follow-up of spontaneous isolated superior mesenteric artery dissection. Eur J Vasc Endovasc Surg. 2009; 37:572–577.29. Nagai T, Torishima R, Uchida A, Nakashima H, Takahashi K, Okawara H, et al. Spontaneous dissection of the superior mesenteric artery in four cases treated with anticoagulation therapy. Intern Med. 2004; 43:473–478.30. Tsuji Y, Hino Y, Sugimoto K, Matsuda H, Okita Y. Surgical intervention for isolated dissecting aneurysm of the superior mesenteric artery--a case report. Vasc Endovascular Surg. 2004; 38:469–472.31. Cho YP, Ko GY, Kim HK, Moon KM, Kwon TW. Conservative management of symptomatic spontaneous isolated dissection of the superior mesenteric artery. Br J Surg. 2009; 96:720–723.32. Wu XM, Wang TD, Chen MF. Percutaneous endovascular treatment for isolated spontaneous superior mesenteric artery dissection: report of two cases and literature review. Catheter Cardiovasc Interv. 2009; 73:145–151.33. Wiesner W, Khurana B, Ji H, Ros PR. CT of acute bowel ischemia. Radiology. 2003; 226:635–650.34. Chou CK, Mak CW, Tzeng WS, Chang JM. CT of small bowel ischemia. Abdom Imaging. 2004; 29:18–22.35. Bakal CW, Sprayregen S, Wolf EL. Radiology in intestinal ischemia. Angiographic diagnosis and management. Surg Clin North Am. 1992; 72:125–114.36. Bauersfeld SR. Dissecting aneurysm of the aorta; a presentation of 15 cases and a review of the recent literature. Ann Intern Med. 1947; 26:873–889.37. Schoots IG, Levi MM, Reekers JA, Lameris JS, van Gulik TM. Thrombolytic therapy for acute superior mesenteric artery occlusion. J Vasc Interv Radiol. 2005; 16:317–329.38. Heiss P, Loewenhardt B, Manke C, Hellinger A, Dietl KH, Schlitt HJ, et al. Primary percutaneous aspiration and thrombolysis for the treatment of acute embolic superior mesenteric artery occlusion. Eur Radiol. 2010; 20:2948–2958.39. Sisteron A, Vieville C. Aneurysmes des arteres a destine digestive: observations personnelles. In : Courbier R, editor. Chirurgle des arteriopathies digestives. Paris: Expansion Scientifique Francaise;1975. p. 197–202. .
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Etiology and Early Treatment Results of Acute Mesenteric Ischemia
- A Case of Inferior Mesenteric Arterial Thrombosis with Bowel Infarction Successfully Treated by Conservative Treatment
- An Unusual Cause of Mesenteric Ischemia of the Small Intestine: Jejunal Neuroendocrine Tumor
- Acute Mesenteric Ischemia after Aortic Valve Replacement: A case report
- A novel hybrid technique to treat flush mesenteric arterial occlusion in acute-on-chronic mesenteric ischemia
